J Clin Neurol.
2009 Mar;5(1):49-52.
Intravenous Recombinant Tissue Plasminogen Activator Thrombolysis in a Patient with Acute Ischemic Stroke Secondary to Aortic Dissection
- Affiliations
-
- 1Department of Neurology, Ilsan Paik Hospital, Inje University College of Medicine, Goyang, Korea. nrhks@paik.ac.kr
- 2Clinical Research Center, Ilsan Paik Hospital, Inje University College of Medicine, Goyang, Korea.
- 3Department of Cardiac Surgery, Ilsan Paik Hospital, Inje University College of Medicine, Goyang, Korea.
Abstract
-
BACKGROUND: Acute ischemic stroke secondary to aortic dissection (AoD) is challenging in the era of thrombolysis owing to the diagnostic difficulty within a narrow time window and the high risk of complications.
CASE REPORT
A 64-year-old woman with middle cerebral artery occlusion syndrome admitted to the emergency room within intravenous recombinant tissue plasminogen activator (rt-PA) time window. Her neurological symptoms improved during thrombolysis, but chest and abdominal pain developed. Repeated history-taking, physical examination, and imaging studies led to the timely diagnosis and surgical treatment of AoD, which produced a successful outcome.
CONCLUSIONS
Clinical suspicion is invaluable for the diagnosis of this rare cause of stroke. Considering the stroke mechanism and complications, the risks of thrombolysis might outweigh its benefits.
MeSH Terms
Figure
-
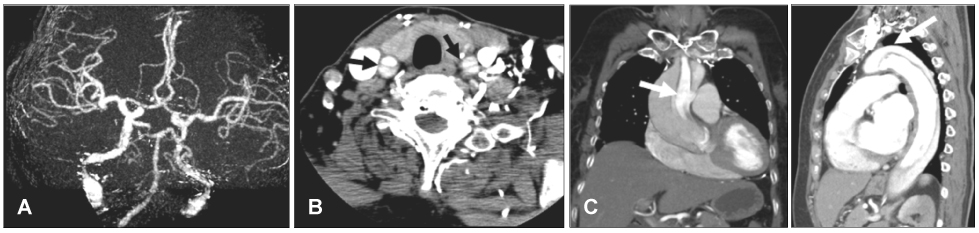
Fig. 1 CT angiography revealed no occlusion in the intracranial major arteries (A), but suggested dissection in the bilateral extracranial carotid arteries on the source images (B, black arrows). Emergent chest CT showed a Stanford type A aortic dissection (C, white arrows).
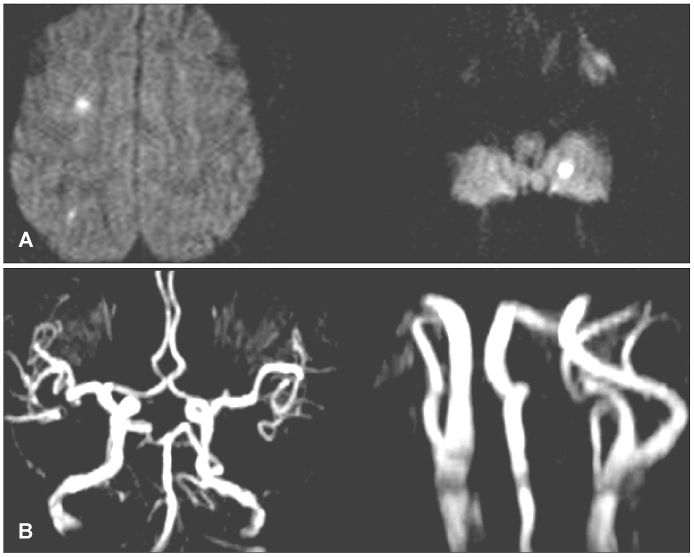
Fig. 2 Follow-up MRI performed 13 days postsurgery revealed small infarctions (A), but no occlusions in the extracranial and intracranial arteries (B).
Reference
-
1. Gaul C, Dietrich W, Friedrich I, Sirch J, Erbguth FJ. Neurological symptoms in type A aortic dissections. Stroke. 2007. 38:292–297.
Article2. Adams HP Jr, del Zoppo G, Alberts MJ, Bhatt DL, Brass L, Furlan A, et al. Guidelines for the early management of adults with ischemic stroke: a guideline from the American Heart Association/American Stroke Association Stroke Council, Clinical Cardiology Council, Cardiovascular Radiology and Intervention Council, and the Atherosclerotic Peripheral Vascular Disease and Quality of Care Outcomes in Research Interdisciplinary Working Groups: the American Academy of Neurology affirms the value of this guideline as an educational tool for neurologists. Stroke. 2007. 38:1655–1711.
Article3. Kamp TJ, Goldschmidt-Clermont PJ, Brinker JA, Resar JR. Myocardial infarction, aortic dissection, and thrombolytic therapy. Am Heart J. 1994. 128:1234–1237.
Article4. Fessler AJ, Alberts MJ. Stroke treatment with tissue plasminogen activator in the setting of aortic dissection. Neurology. 2000. 54:1010.
Article5. Ibaraki T, Fukumoto H, Nishimoto Y, Nishimoto M, Suzuki S, Morita H. [Surgical management of acute type A aortic dissection with a complaint of disturbance of consciousness; report of a case]. Kyobu Geka. 2002. 55:1053–1056.6. Chua CH, Lien LM, Lin CH, Hung CR. Emergency surgical intervention in a patient with delayed diagnosis of aortic dissection presenting with acute ischemic stroke and undergoing thrombolytic therapy. J Thorac Cardiovasc Surg. 2005. 130:1222–1224.
Article7. Uchino K, Estrera A, Calleja S, Alexandrov AV, Garami Z. Aortic dissection presenting as an acute ischemic stroke for thrombolysis. J Neuroimaging. 2005. 15:281–283.
Article8. Flemming KD, Brown RD Jr. Acute cerebral infarction caused by aortic dissection: caution in the thrombolytic era. Stroke. 1999. 30:477–478.
Article9. Villa A, Molgora M, Licari S, Omboni E. Acute ischemic stroke, aortic dissection, and thrombolytic therapy. Am J Emerg Med. 2003. 21:159–160.
Article10. Wright V, Horvath R, Baird AE. Aortic dissection presenting as acute ischemic stroke. Neurology. 2003. 61:581–582.
Article11. Grupper M, Eran A, Shifrin A. Ischemic stroke, aortic dissection, and thrombolytic therapy--the importance of basic clinical skills. J Gen Intern Med. 2007. 22:1370–1372.
Article12. Yeh JF, Po H, Chien CY. Ischaemic infarction masking aortic dissection: a pitfall to be avoided before thrombolysis. Emerg Med J. 2007. 24:594–595.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Aortic Dissection after Intravenous Thrombolysis in Acute Cerebral Infarction
- Unexpected Complication of Intravenous Recombinant Tissue Plasminogen Activator Thrombolysis in a Patient with Acute Ischemic Stroke: Aortic Dissection
- Treatment of Acute Ischemic Stroke: Thrombolysis
- Delayed Surgery for Aortic Dissection after Intravenous Thrombolysis in Acute Ischemic Stroke
- Intravenous Thrombolysis and Endovascular Thrombectomy in Acute Ischemic Stroke with Minor Symptom
