Kosin Med J.
2017 Jun;32(1):127-132. 10.7180/kmj.2017.32.1.127.
Aortic Dissection after Intravenous Thrombolysis in Acute Cerebral Infarction
- Affiliations
-
- 1Department of Neurology, Catholic University of Daegu School of Medicine, Daegu, Korea. dyr4173@cu.ac.kr
- KMID: 2384842
- DOI: http://doi.org/10.7180/kmj.2017.32.1.127
Abstract
- Use of recombinant tissue plasminogen activator (rt-PA) for the treatment of acute cerebral infarction secondary to aortic dissection is challenging because of a narrow time window and potential life-threatening complications. An 80-year-old woman with right middle cerebral artery infarction was treated with rt-PA. Although she had no history, symptoms, or sign of aortic dissection, carotid CT angiography revealed aortic arch dissection. Mediastinal widening, which did not show on initial chest X-ray, developed on follow-up chest X-ray. This observation indicates that physicians should monitor patient symptoms for signs of aortic dissection during thrombolysis and perform chest X-ray or carotid angiography immediately after thrombolysis even if the patient has no symptoms or signs of aortic dissection on onset of acute cerebral infarction.
MeSH Terms
Figure
-
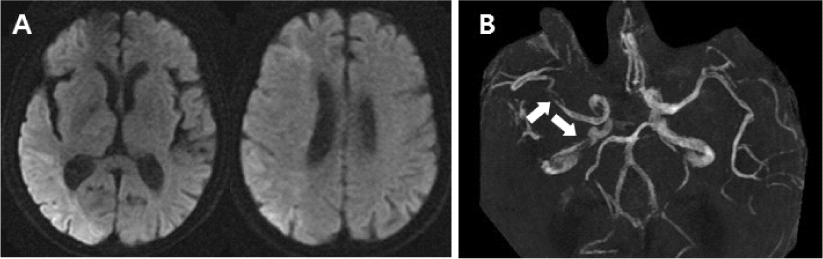
Fig. 1 MR diffusion weighted images (A) and MR angiography (B) shows acute right hemispheric infarction with stenosis of the right middle cerebral artery and intracranial internal carotid artery (white arrows).

Fig. 2 Comparing with unremarkable initial chest X-ray (A), followed-up chest X-ray revealed mediastinal widening (B, black arrowheads).
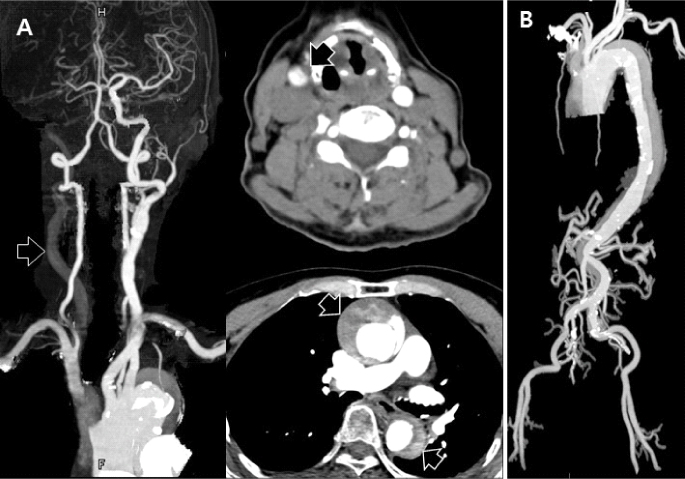
Fig. 3 Carotid (A) and aorta CT angiography (B) shows that aortic dissection (Stanford A, DeBakey I) with the occlusion ofthe right common carotid artery (black arrows).
Cited by 1 articles
-
Neurovascular Complications of Acute Aortic Syndrome
Dean Zeldich, Matthew Bierowski, Leah Shabo, Sridhara Yaddanapudi, Gregary Marhefka
J Stroke. 2025;27(1):19-29. doi: 10.5853/jos.2024.02915.
Reference
-
1. Marian AJ, Harris SL, Pickett JD, Campbell E, Fromm RE. Inadvertent administration of rtPA to a patient with type 1 aortic dissection and subsequent cardiac tamponade. Am J Emerg Med. 1993; 11:613–615.
Article2. Tsigkas G, Kasimis G, Theodoropoulos K, Chouchoulis K, Baikoussis NG, Aopstolakis E, et al. A successfully thrombolysed acute inferior myocardial infarction due to type A aortic dissection with lethal consequences: the importance of early cardiac echocardiography. J Cardiothorac Surg. 2011; 6:101.
Article3. Grupper M, Eran A, Shifrin A. Ischemic stroke, aortic dissection, and thrombolytic therapy--the importance of basic clinical skills. J Gen Intern Med. 2007; 22:1370–1372.
Article4. Hong KS, Park SY, Whang SI, Seo SY, Lee DH, Kim HJ, et al. Intravenous recombinant tissue plasminogen activator thrombolysis in a patient with acute ischemic stroke secondary to aortic dissection. J Clin Neurol. 2009; 5:49–52.
Article5. Ramalingam VS, Sinnakirouchenan R, Sudhakar S, Brasch AV. Acute ischemic stroke in aortic dissection: case report and review of literature. Indian J Med Sci. 2010; 64:385–389.
Article6. Demaerschalk BM, Kleindorfer DO, Adeoye OM, Demchuk AM, Fugate JE, Grotta JC, et al. Scientific Rationale for the Inclusion and Exclusion Criteria for Intravenous Alteplase in Acute Ischemic Stroke: A Statement for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke. 2016; 47:581–641.
Article7. Fessler AJ, Alberts MJ. Stroke treatment with tissue plasminogen activator in the setting of aortic dissection. Neurology. 2000; 54:1010.
Article8. Villa A, Molgora M, Licari S, Omboni E. Acute ischemic stroke, aortic dissection, and thrombolytic therapy. Am J Emerg Med. 2003; 21:159–160.
Article9. Yamashiro S, Arakaki R, Kise Y, Kuniyoshi Y. Emergency operation for aortic dissection with ischemic stroke. Asian Cardiovasc Thorac Ann. 2014; 22:208–211.
Article10. Hama Y, Koga M, Tokunaga K, Takizawa H, Miyashita K, Iba Y, et al. Carotid Ultrasonography Can Identify Stroke Patients Ineligible for Intravenous Thrombolysis Therapy due to Acute Aortic Dissection. J Neuroimaging. 2015; 25:671–673.
Article11. Matsumoto H, Yoshida Y, Hirata Y. Usefulness of cervical magnetic resonance imaging for detecting type A acute aortic dissection with acute stroke symptoms. Magn Reson Imaging. 2016; 34:902–907.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Rare Cerebral Infarction in Patient with Type B Aortic Dissection
- Renal Subcapsular Hematoma after Intravenous Thrombolysis in a Patient with Acute Cerebral Infarction
- Cerebral Infarction Caused by Painless Aortic Dissection
- Delayed Surgery for Aortic Dissection after Intravenous Thrombolysis in Acute Ischemic Stroke
- Unexpected Complication of Intravenous Recombinant Tissue Plasminogen Activator Thrombolysis in a Patient with Acute Ischemic Stroke: Aortic Dissection
