Alveolar ridge preservation with an open-healing approach using single-layer or double-layer coverage with collagen membranes
- Affiliations
-
- 1Department of Periodontology, Dankook University College of Dentistry, Cheonan, Korea. periopark@dankook.ac.kr
- 2Department of Periodontology, Seoul National University School of Dentistry, Seoul, Korea.
- 3Clinic for Fixed and Removable Prosthodontics and Dental Material Science, University of Zurich, Zurich, Switzerland.
- KMID: 2399743
- DOI: http://doi.org/10.5051/jpis.2017.47.6.372
Abstract
- PURPOSE
The aim of this prospective pilot study was to compare alveolar ridge preservation (ARP) procedures with open-healing approach using a single-layer and a double-layer coverage with collagen membranes using radiographic and clinical analyses.
METHODS
Eleven molars from 9 healthy patients requiring extraction of the maxillary or mandibular posterior teeth were included and allocated into 2 groups. After tooth extraction, deproteinized bovine bone mineral mixed with 10% collagen was grafted into the socket and covered either with a double-layer of resorbable non-cross-linked collagen membranes (DL group, n=6) or with a single-layer (SL group, n=5). Primary closure was not obtained. Cone-beam computed tomography images were taken immediately after the ARP procedure and after a healing period of 4 months before implant placement. Radiographic measurements were made of the width and height changes of the alveolar ridge.
RESULTS
All sites healed without any complications, and dental implants were placed at all operated sites with acceptable initial stability. The measurements showed that the reductions in width at the level 1 mm apical from the alveolar crest (including the bone graft) were −1.7±0.5 mm in the SL group and −1.8±0.4 mm in the DL group, and the horizontal changes in the other areas were also similar in the DL and SL groups. The reductions in height were also comparable between groups.
CONCLUSIONS
Within the limitations of this study, single-layer and double-layer coverage with collagen membranes after ARP failed to show substantial differences in the preservation of horizontal or vertical dimensions or in clinical healing. Thus, both approaches seem to be suitable for open-healing ridge preservation procedures.
MeSH Terms
Figure
-
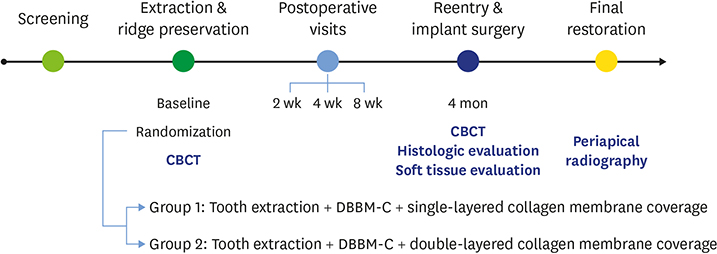
Figure 1 Schematic presentation of the study schedule and design. CBCT: cone-beam computed tomography, DBBM-C: deproteinized bovine bone mineral with 10% porcine collagen.
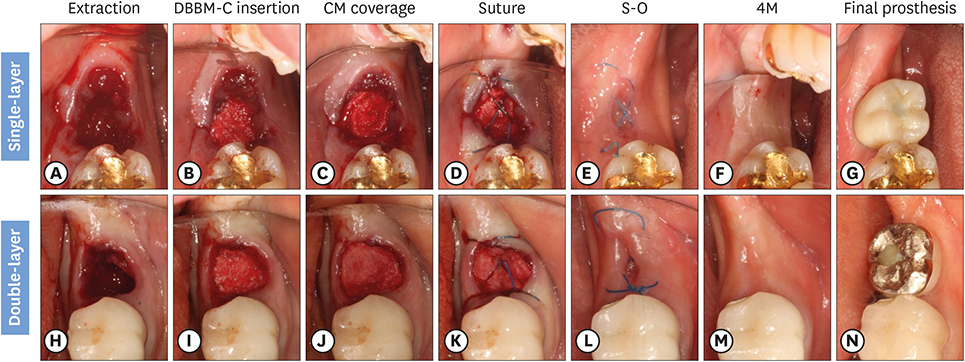
Figure 2 Surgical procedures of the SL and DL open membrane healing technique. The procedures of the SL and DL groups were only different in the number of the resorbable collagen membranes used to cover the bone graft. (A) Extraction in the SL group. (B) DBBM-C insertion in the SL group. (C) Single-layer of collagen membrane coverage in the SL group. (D) The hidden X or the figure of 8 suture in the SL group. (E) Just before S-O. (F) Four months after extraction, immediately followed by dental implant placement. (G) Occlusal view of the final prosthesis. (H) Extraction in the DL group. (I) DBBM-C insertion in the DL group. (J) Double-layers of collagen membrane coverage in the DL group. (K) The hidden X or the figure of 8 suture in the DL group. (L) Just before S-O. (M) Four months after extraction, immediately followed by dental implant placement in the DL group. (N) Occlusal view of the final prosthesis in the DL group. SL: the socket was filled with deproteinized bovine bone mineral with 10% collagen and covered by a single-layer of a collagen membrane, DL: the socket was filled with deproteinized bovine bone mineral with 10% collagen and covered by a double-layer of a collagen membrane, DBBM-C: deproteinized bovine bone mineral with 10% porcine collagen, S-O: stitch-out, 4M: 4 months after alveolar ridge preservation procedure.
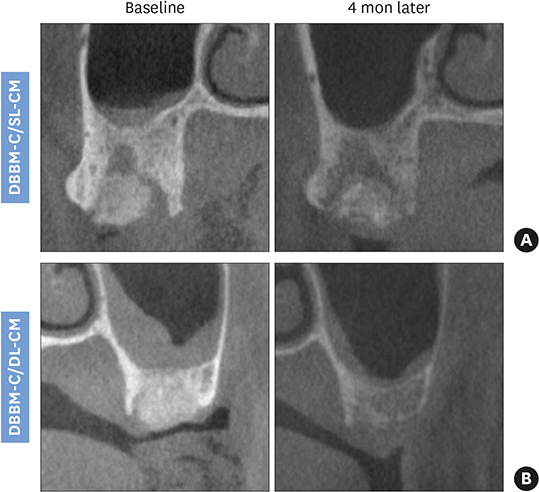
Figure 3 Paraxial views from CBCT obtained 4 months after SL (A) and DL (B) ARP procedures. CBCT: cone-beam computed tomography, SL: the socket was filled with deproteinized bovine bone mineral with 10% collagen and covered by a single-layer of a collagen membrane, DL: the socket was filled with deproteinized bovine bone mineral with 10% collagen and covered by a double-layer of a collagen membrane, ARP: alveolar ridge preservation, DBBM-C: deproteinized bovine bone mineral with 10% porcine collagen, CM: collagen membrane.
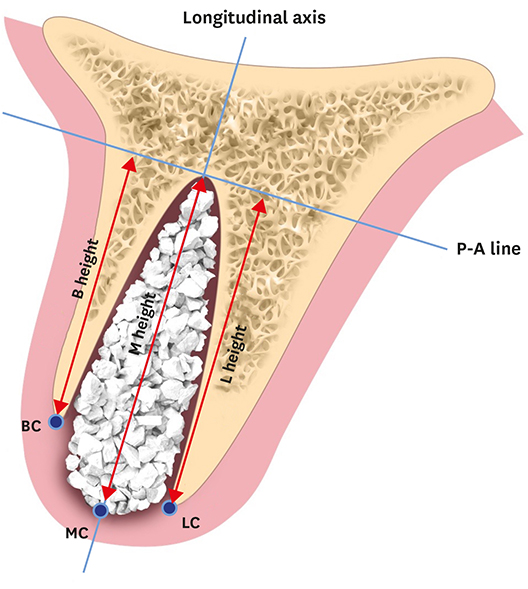
Figure 4 Schematic drawing of references for measurements in the radiographic analysis. P-A line: perpendicular line to the longitudinal axis at apex of the socket, BC: buccal crest, B height: height of the buccal cortical plate from the P-A line, LC: lingual/palatal crest, L height: height of the lingual/palatal plate from the P-A line, MC: mid-alveolar crest, M height: height of the mid-alveolar crest from the P-A line.
Reference
-
1. Tallgren A. The continuing reduction of the residual alveolar ridges in complete denture wearers: a mixed-longitudinal study covering 25 years. J Prosthet Dent. 1972; 27:120–132.
Article2. Atwood DA. Reduction of residual ridges: a major oral disease entity. J Prosthet Dent. 1971; 26:266–279.
Article3. Schropp L, Wenzel A, Kostopoulos L, Karring T. Bone healing and soft tissue contour changes following single-tooth extraction: a clinical and radiographic 12-month prospective study. Int J Periodontics Restorative Dent. 2003; 23:313–323.4. Araújo MG, Lindhe J. Dimensional ridge alterations following tooth extraction. An experimental study in the dog. J Clin Periodontol. 2005; 32:212–218.
Article5. Tan WL, Wong TL, Wong MC, Lang NP. A systematic review of post-extractional alveolar hard and soft tissue dimensional changes in humans. Clin Oral Implants Res. 2012; 23:Suppl 5. 1–21.
Article6. Kentros GA, Filler SJ, Rothstein SS. Six month evaluation of particulate Durapatite in extraction sockets for the preservation of the alveolar ridge. Implantologist. 1985; 3:53–62.7. Cohen ES. Ridge enhancement and socket preservation utilizing the subepithelial connective tissue graft: a case report. Pract Periodontics Aesthet Dent. 1995; 7:53–58.8. Artzi Z, Nemcovsky CE. The application of deproteinized bovine bone mineral for ridge preservation prior to implantation. Clinical and histological observations in a case report. J Periodontol. 1998; 69:1062–1067.
Article9. Cardaropoli D, Cardaropoli G. Preservation of the postextraction alveolar ridge: a clinical and histologic study. Int J Periodontics Restorative Dent. 2008; 28:469–477.10. Araújo MG, Lindhe J. Ridge alterations following tooth extraction with and without flap elevation: an experimental study in the dog. Clin Oral Implants Res. 2009; 20:545–549.
Article11. Roccuzzo M, Gaudioso L, Bunino M, Dalmasso P. Long-term stability of soft tissues following alveolar ridge preservation: 10-year results of a prospective study around nonsubmerged implants. Int J Periodontics Restorative Dent. 2014; 34:795–804.
Article12. Mardas N, Chadha V, Donos N. Alveolar ridge preservation with guided bone regeneration and a synthetic bone substitute or a bovine-derived xenograft: a randomized, controlled clinical trial. Clin Oral Implants Res. 2010; 21:688–698.
Article13. Engler-Hamm D, Cheung WS, Yen A, Stark PC, Griffin T. Ridge preservation using a composite bone graft and a bioabsorbable membrane with and without primary wound closure: a comparative clinical trial. J Periodontol. 2011; 82:377–387.
Article14. Pellegrini G, Rasperini G, Obot G, Farronato D, Dellavia C. Soft tissue healing in alveolar socket preservation technique: histologic evaluations. Int J Periodontics Restorative Dent. 2014; 34:531–539.
Article15. Barone A, Toti P, Piattelli A, Iezzi G, Derchi G, Covani U. Extraction socket healing in humans after ridge preservation techniques: comparison between flapless and flapped procedures in a randomized clinical trial. J Periodontol. 2014; 85:14–23.
Article16. Park JC, Koo KT, Lim HC. The hidden X suture: a technical note on a novel suture technique for alveolar ridge preservation. J Periodontal Implant Sci. 2016; 46:415–425.
Article17. Cho IW, Park JC, Shin HS. A comparison of different compressive forces on graft materials during alveolar ridge preservation. J Periodontal Implant Sci. 2017; 47:51–63.
Article18. Buser D, Martin W, Belser UC. Optimizing esthetics for implant restorations in the anterior maxilla: anatomic and surgical considerations. Int J Oral Maxillofac Implants. 2004; 19:Suppl. 43–61.19. von Arx T, Buser D. Horizontal ridge augmentation using autogenous block grafts and the guided bone regeneration technique with collagen membranes: a clinical study with 42 patients. Clin Oral Implants Res. 2006; 17:359–366.
Article20. Kim SH, Kim DY, Kim KH, Ku Y, Rhyu IC, Lee YM. The efficacy of a double-layer collagen membrane technique for overlaying block grafts in a rabbit calvarium model. Clin Oral Implants Res. 2009; 20:1124–1132.
Article21. Zitzmann NU, Naef R, Schärer P. Resorbable versus nonresorbable membranes in combination with Bio-Oss for guided bone regeneration. Int J Oral Maxillofac Implants. 1997; 12:844–852.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Re-implantation at a Failed Site Using Alveolar Ridge Preservation with Open-healing Approach: A 5-year Follow-up
- Immediate Implant Placement with Open Healing Alveolar Ridge Preservation in the Molar Region: A Case Report
- The influence of membrane exposure on post-extraction dimensional change following ridge preservation technique
- The hidden X suture: a technical note on a novel suture technique for alveolar ridge preservation
- Role of collagen membrane in lateral onlay grafting with bovine hydroxyapatite incorporated with collagen matrix in dogs
