Asia Pac Allergy.
2014 Jul;4(3):180-183. 10.5415/apallergy.2014.4.3.180.
Successful wheat-specific oral immunotherapy in highly sensitive individuals with a novel multirush/maintenance regimen
- Affiliations
-
- 1Division of Allergy and Immunology, Department of Pediatrics, Siriraj Hospital, Mahidol University Faculty of Medicine, Bangkok 10700, Thailand. punchama@gmail.com
- KMID: 2397097
- DOI: http://doi.org/10.5415/apallergy.2014.4.3.180
Abstract
- We reported a successful oral immunotherapy (OIT) in 2 children with high wheat sensitivity (4 and 14 years old boys). Oral challenges indicated eliciting doses of 300 mg, and wheat flour of 30 mg. The OIT protocol includes 5 days of build-up phase in the hospital, intervening with 2 to 5 months of home maintenance phase. Patients could tolerate 45 g, and 60 g of wheat flour per day, respectively. We have demonstrated that OIT to a large amount of wheat in extremely sensitized patients could be achieved with a stepwise multi oral/maintenance regimen.
Keyword
Figure
-

Fig. 1 (A) Oral immunotherapy (OIT) protocol of patient #1. (B) Protocol of patient #2. U, urticarial; B, bronchospasm; C, cyanosis; E, edema; H, hoarseness; R, rash; Ad, adrenaline; An, antihistamine; Ab, abdominal pain; P, prednisolone; F, flushing; No, no treatment; IgE, immunoglobulin E.
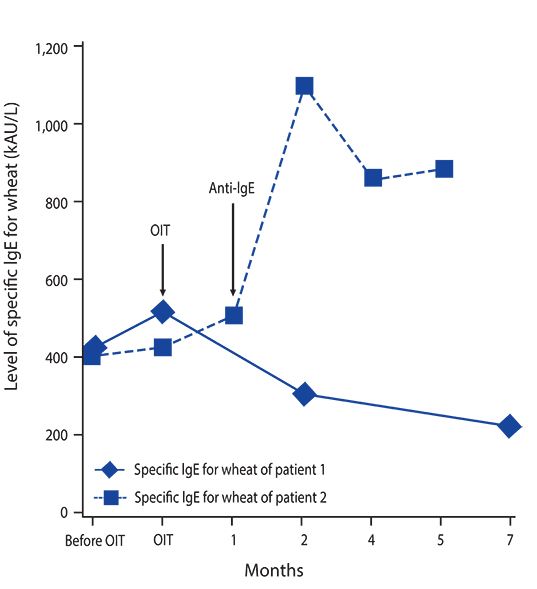
Fig. 2 Level of specific immunoglobulin E (IgE) for wheat of 2 patients. OIT, oral immunotherapy.
Reference
-
1. Sampson HA. Food allergy. Part 2: diagnosis and management. J Allergy Clin Immunol. 1999; 103:981–989.
Article2. Keet CA, Matsui EC, Dhillon G, Lenehan P, Paterakis M, Wood RA. The natural history of wheat allergy. Ann Allergy Asthma Immunol. 2009; 102:410–415.
Article3. Vickery BP, Burks W. Oral immunotherapy for food allergy. Curr Opin Pediatr. 2010; 22:765–770.
Article4. Longo G, Barbi E, Berti I, Meneghetti R, Pittalis A, Ronfani L, Ventura A. Specific oral tolerance induction in children with very severe cow's milk-induced reactions. J Allergy Clin Immunol. 2008; 121:343–347.
Article5. García Rodríguez R, Urra JM, Feo-Brito F, Galindo PA, Borja J, Gomez E, Lara P, Guerra F. Oral rush desensitization to egg: efficacy and safety. Clin Exp Allergy. 2011; 41:1289–1296.
Article6. Fujino A, Kurihara K. Two cases of rush specific oral tolerance induction for wheat allergy. Arerugi. 2010; 59:1580–1584.7. Leung DY, Sampson HA, Yunginger JW, Burks AW Jr, Schneider LC, Wortel CH, Davis FM, Hyun JD, Shanahan WR Jr. Avon Longitudinal Study of Parents and Children Study Team. Effect of anti-IgE therapy in patients with peanut allergy. N Engl J Med. 2003; 348:986–993.
Article8. Nadeau KC, Schneider LC, Hoyte L, Borras I, Umetsu DT. Rapid oral desensitization in combination with omalizumab therapy in patients with cow's milk allergy. J Allergy Clin Immunol. 2011; 127:1622–1624.
Article9. Burks AW, Jones SM, Wood RA, Fleischer DM, Sicherer SH, Lindblad RW, Stablein D, Henning AK, Vickery BP, Liu AH, Scurlock AM, Shreffler WG, Plaut M, Sampson HA. Consortium of Food Allergy Research (CoFAR). Oral immunotherapy for treatment of egg allergy in children. N Engl J Med. 2012; 367:233–243.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Real-world cases with wheat oral immunotherapy in children with multiple food anaphylaxis
- Update of immunoglobulin E-mediated wheat allergy
- Usefulness of specific IgE antibody levels to wheat, gluten, and ω-5 gliadin for wheat allergy in Korean children
- The effect of house dust mite conventional immunotherapy on the production of IL-4 and interferon-gamma from the peripheral blood T cells in asthmatic children
- Wheat-Induced Anaphylaxis in Korean Adults: A Report of 6 Cases
