Yonsei Med J.
2008 Feb;49(1):138-143.
The Relationship between Aldosterone to Renin Ratio and RI Value of the Uterine Artery in the Preeclamptic Patient vs. Normal Pregnancy
- Affiliations
-
- 1Department of Obstetrics and Gynecology, Yonsei University College of Medicine, Seoul, Korea. ob@yuhs.ac
Abstract
- PURPOSE
Plasma levels of renin, angiotensin II and aldosterone are increased during normal pregnancy. However, these values in preeclampsia are decreased to nearly that of a nonpregnant subject, and vascular sensitivity to angiotensin II is increased. In preeclampsia, aldosterone is decreased less than rennin. Therefore current studies were undertaken to determine the relationship between aldosterone to renin ratio (ARR) and uterine artery perfusion via RI value. MATERIALS AND METHODS: In this study, the relationship between plasma aldosterone and renin concentration was determined in 27 preeclamptic women and 50 normal pregnant women, whose gestational weeks were matched. The aldosterone to renin ratio was calculated and compared between the two groups. Doppler velocimetry of the uterine artery, which was used to calculate resistance index (RI), was performed on all subjects. The relationship between ARR and RI value was reviewed. RESULTS: In the preeclampsia group, RI value of the uterine artery was significantly higher than that of normal pregnant women. Both plasma renin and aldosterone concentrations were lower in the preeclampsia group. However, the ratio of these two parameters was significantly higher (38.3 vs. 16.1, p < 0.001); the greater ARR, the higher the RI of the uterine artery (r(2)=0.053, p=0.048). CONCLUSION: This study demonstrates that a high aldosterone to renin ratio may have a negative effect on perfusion of the uterine artery and play an important role in the pathophysiology of preeclampsia.
Keyword
MeSH Terms
Figure
-

Fig. 1 Correlation between gestational age and renin (r=0.18, p = 0.11).
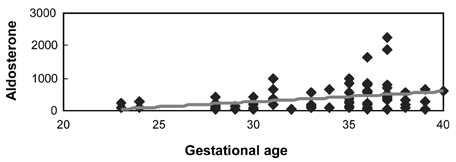
Fig. 2 Correlation between gestational age and aldosterone (r=0.33, p = 0.003).
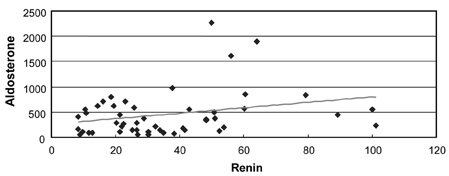
Fig. 3 Correlation between renin and aldosterone in normal pregnancy (r=0.3, p = 0.04).
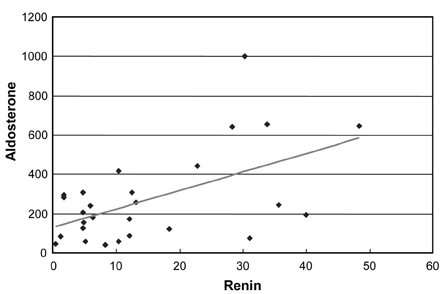
Fig. 4 Correlation between renin and aldosterone in preeclampsia (r=0.55, p = 0.003).
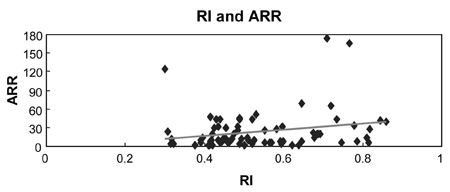
Fig. 5 Correlation between RI and ARR (r=0.23, p = 0.048).
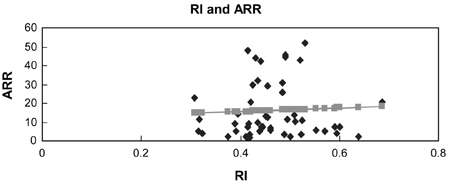
Fig. 6 Control group (r=0.052, p = 0.718).
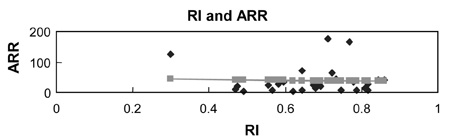
Fig. 7 Preeclampsia group (r=0.033, p = 0.868).
Reference
-
1. Gladstone IM, Katz VL. The morbidity of the 34-to 35-week gestation: should we reexamine the paradigm? Am J Perinatol. 2004. 21:9–13.
Article2. Meekins JW, Pijnenborg R, Hanssens M, McFadyen IR, van Asshe A. A study of placental bed spiral arteries and trophoblast invasion in normal and severe pre-eclamptic pregnancies. Br J Obstet Gynaecol. 1994. 101:669–674.
Article3. Weir RJ, Brown JJ, Fraser R, Kraszewski A, Lever AF, McIlwaine GM, et al. Plasma renin, renin substrate, angiotensin II, and aldosterone in hypertensive disease of pregnancy. Lancet. 1973. 1:291–294.
Article4. Brown MA, Zammit VC, Mitar DA, Whitworth JA. Renin-aldosterone relationships in pregnancy-induced hypertension. Am J Hypertens. 1992. 5(6 Pt 1):366–371.5. Mahmud A, Feely J. Aldosterone-to-renin ratio, arterial stiffness, and the response to aldosterone antagonism in essential hypertension. Am J Hypertens. 2005. 18:50–55.
Article6. Thaler I, Weiner Z, Itskovitz J. Systolic or diastolic notch in uterine artery blood flow velocity waveforms in hypertensive pregnant patients: relationship to outcome. Obstet Gynecol. 1992. 80:277–282.7. Elsheikh A, Creatsas G, Mastorakos G, Milingos S, Loutradis D, Michalas S. The rennin-aldosterone system during normal and hypertensive pregnancy. Arch Gynecol Obstet. 2001. 264(4):182–185.8. Shah DM. Role of the renin-angiotensin system in the pathogenesis of preeclampsia. Am J Physiol Renal Physiol. 2005. 288:F614–F625.
Article9. Dzau VJ, Gonzalez D, Ellison K, Churchill S, Emmett N. Characterization of purified rabbit uterine renin: influence of pregnancy on uterine inactive renin. Endocrinology. 1987. 120:358–364.
Article10. Kaplan NM, Lieberman E, Neal W. Hypertension with pregnancy and the pill. Kaplan's clinical hypertension. 2002. 8th ed. Philadelphia: Lippincott Williams & Wilkins;404–433. Chapt 11.11. Ochi H, Matsubara K, Kusanagi Y, Taniguchi H, Ito M. Significance of a diastolic notch in the uterine artery flow velocity waveform induced by uterine embolisation in the pregnant ewe. Br J Obstet Gynaecol. 1998. 105:1118–1121.
Article12. Gant NF, Worley RJ, Everett RB, MacDonald PC. Control of vascular responsiveness during human pregnancy. Kidney Int. 1980. 18:253–258.
Article13. Forcier I, St-Louis J, Brochu M. Angiotensin II receptor subtypes in the adrenals of pregnant rats. Mol Cell Endocrinol. 1995. 114:177–186.
Article14. August P, Lenz T, Ales KL, Druzin ML, Edersheim TG, Hutson JM, et al. Longitudinal study of the renin-angiotensin-aldosterone system in hypertensive pregnant women: deviations related to the development of superimposed preeclampsia. Am J Obstet Gynecol. 1990. 163(5 Pt 1):1612–1621.
Article15. Chung JE, Cho JS, Han SS, Park YW, Kim JW. Uterine artery Doppler velocimetry in the prediction of adverse obstetric outcomes in unexplained MSAFP elevations. Yonsei Med J. 2000. 41:17–21.
Article16. Maulik D. Hemodynamic interpretation of the arterial Doppler waveform. Ultrasound Obstet Gynecol. 1993. 3:219–227.
Article17. Israel A, Peceño A. Renin-angiotensin-aldosterone system in pregnancy-induced hypertension. J Hum Hypertens. 2000. 14 :Suppl 1. S36–S39.
Article18. Brochu M, Lehoux JG, Picard S. Effects of gestation on enzymes controlling aldosterone synthesis in the rat adrenal. Endocrinology. 1997. 138:2354–2358.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Transvaginal Color Doppler Imaging in the Assessment of Utero-placental Blood Flow in Normal and Abnormal Early Pregnany
- Pulsatility Index of Renal Artery in Patients with Liver Cirrhosis
- A study of plasma renin activity and plasma aldosterone in chronic liver diseases
- A Study on the Change of Plasma Renin Activity(PRA) and Aldosterone Concentration(PAC) before and after Heart Operation in Children with Congenital Heart Disease
- Two Cases with Pseudohypoaldosteronism
