Ann Surg Treat Res.
2017 Nov;93(5):260-265. 10.4174/astr.2017.93.5.260.
Three-year result of efficacy for type 2 diabetes mellitus control between laparoscopic duodenojejunal bypass compared with laparoscopic Roux-en-Y gastric bypass
- Affiliations
-
- 1Department of Surgery, Yeouido St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea. kimwook@catholic.ac.kr
- 2Department of Endocrinology, Yeouido St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea.
- KMID: 2393991
- DOI: http://doi.org/10.4174/astr.2017.93.5.260
Abstract
- PURPOSE
The mechanism by which bariatric surgery facilitates diabetic control is still unknown. Duodenojejunal bypass supports the foregut theory; however, its efficacy when used alone is not yet established.
METHODS
During the period from January 2008 to December 2009, patients who underwent laparoscopic duodenojejunal bypass (LDJB) or laparoscopic Roux-en-Y gastric bypass (LRYGB) for type 2 diabetes mellitus (T2DM) with or without morbid obesity were included. Patients who had a follow-up for less than 3 years were excluded. Patient baseline characteristics, change of body weight, body mass index (BMI), glycosylated hemoglobin (HbA1c), and diabetic treatments were analyzed.
RESULTS
In total, 8 LDJB and 20 LRYGB patients were analyzed. The LDJB group had more number of male patients than the LRYGB group (LDJB 75% vs. LRYGB 30%, P = 0.030). Baseline BMI in the LRYGB group was higher than in the LDJB group (LDJB 27.0 ± 2.5 vs. LRYGB 32.6 ± 3.4, P < 0.001). Age, DM duration, baseline HbA1c, and C-peptide levels were similar. Longer operation time was needed to perform LDJB (LDJB 367.5 ± 120.2 vs. LRYGB 232.9 ± 41.1, P < 0.001), but no differences were observed in the hospital stay and complication rate between the 2 groups. At the third year of follow-up, the T2DM remission rate was observed in 40% of patients in the LRYGB group and 12.5% of patients in the LDJB group.
CONCLUSION
LDJB is not an effective method for controlling T2DM compared with LRYGB. Foregut theory may not be the main mechanism of diabetic control during bariatric surgery.
Keyword
MeSH Terms
Figure
-

Fig. 1 Illustration for the duodeno-jejunal bypass.
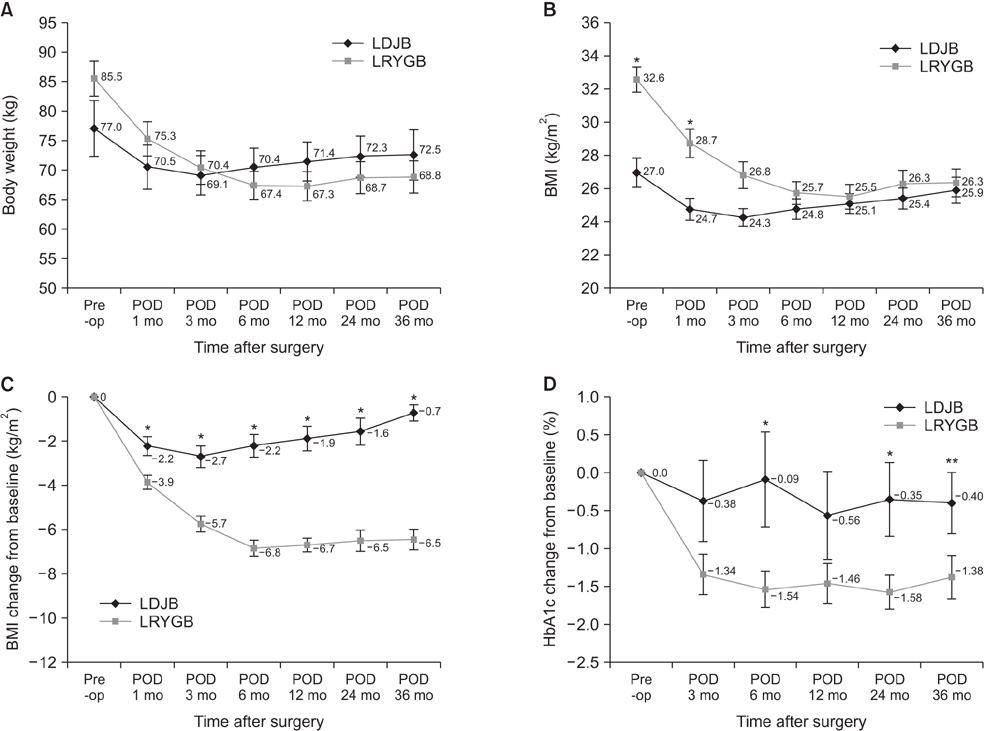
Fig. 2 Body weight change from preoperative period to postoperative third year (A), body mass index (BMI) change from preoperative period to postoperative third year (B), change of BMI difference from the baseline BMI (C), change of glycosylated hemoglobin (HbA1c) difference from the baseline HbA1c (D). *P < 0.05. **P < 0.1.
Reference
-
1. Heo Y, Ahn JH, Shin SH, Lee YJ. The effect of duodenojejunal bypass for type 2 diabetes mellitus patients below body mass index 25 kg/m(2): one year follow-up. J Korean Surg Soc. 2013; 85:109–115.2. Wild S, Roglic G, Green A, Sicree R, King H. Global prevalence of diabetes: estimates for the year 2000 and projections for 2030. Diabetes Care. 2004; 27:1047–1053.3. Ntuk UE, Gill JM, Mackay DF, Sattar N, Pell JP. Ethnic-specific obesity cutoffs for diabetes risk: cross-sectional study of 490,288 UK biobank participants. Diabetes Care. 2014; 37:2500–2507.4. Lee HJ, Ahn HS, Choi YB, Han SM, Han SU, Heo YS, et al. Nationwide survey on bariatric and metabolic surgery in Korea: 2003-2013 Results. Obes Surg. 2016; 26:691–695.5. Park JY, Kim YJ. Laparoscopic sleeve gastrectomy in obese Korean patients: up to 4-year follow-up in a single center. Ann Surg Treat Res. 2015; 88:246–252.6. Mingrone G, Panunzi S, De Gaetano A, Guidone C, Iaconelli A, Leccesi L, et al. Bariatric surgery versus conventional medical therapy for type 2 diabetes. N Engl J Med. 2012; 366:1577–1585.7. Laferrere B, Teixeira J, McGinty J, Tran H, Egger JR, Colarusso A, et al. Effect of weight loss by gastric bypass surgery versus hypocaloric diet on glucose and incretin levels in patients with type 2 diabetes. J Clin Endocrinol Metab. 2008; 93:2479–2485.8. Rubino F, Forgione A, Cummings DE, Vix M, Gnuli D, Mingrone G, et al. The mechanism of diabetes control after gastrointestinal bypass surgery reveals a role of the proximal small intestine in the pathophysiology of type 2 diabetes. Ann Surg. 2006; 244:741–749.9. Ferzli GS, Dominique E, Ciaglia M, Bluth MH, Gonzalez A, Fingerhut A. Clinical improvement after duodenojejunal bypass for nonobese type 2 diabetes despite minimal improvement in glycemic homeostasis. World J Surg. 2009; 33:972–979.10. Paik KY, Kim W, Song KH, Kwon HS, Kim MK, Kim E. The preliminary clinical experience with laparoscopic duodeno-jejunal bypass for treatment of type 2 diabetes mellitus in non-morbidly obese patients: the 1-year result in a single institute. Surg Endosc. 2012; 26:3287–3292.11. Rubino F, Marescaux J. Effect of duodenal-jejunal exclusion in a non-obese animal model of type 2 diabetes: a new perspective for an old disease. Ann Surg. 2004; 239:1–11.12. Gersin KS, Rothstein RI, Rosenthal RJ, Stefanidis D, Deal SE, Kuwada TS, et al. Open-label, sham-controlled trial of an endoscopic duodenojejunal bypass liner for preoperative weight loss in bariatric surgery candidates. Gastrointest Endosc. 2010; 71:976–982.13. de Moura EG, Orso IR, Martins BC, Lopes GS, de Oliveira SL, Galvao-Neto Mdos P, et al. Improvement of insulin resistance and reduction of cardiovascular risk among obese patients with type 2 diabetes with the duodenojejunal bypass liner. Obes Surg. 2011; 21:941–947.14. Woods M, Lan Z, Li J, Wheeler MB, Wang H, Wang R. Antidiabetic effects of duodenojejunal bypass in an experimental model of diabetes induced by a high-fat diet. Br J Surg. 2011; 98:686–696.15. Buchwald H. Consensus Conference Panel. Consensus conference statement bariatric surgery for morbid obesity: health implications for patients, health professionals, and third-party payers. Surg Obes Relat Dis. 2005; 1:371–381.16. Huang CK, Goel R, Tai CM, Yen YC, Gohil VD, Chen XY. Novel metabolic surgery for type II diabetes mellitus: loop duodenojejunal bypass with sleeve gastrectomy. Surg Laparosc Endosc Percutan Tech. 2013; 23:481–485.17. Seki Y, Kasama K, Haruta H, Watanabe A, Yokoyama R, Porciuncula JP, et al. Five-year-results of laparoscopic sleeve gastrectomy with duodenojejunal bypass for weight loss and type 2 diabetes mellitus. Obes Surg. 2017; 27:795–801.18. Lee WJ, Almulaifi AM, Tsou JJ, Ser KH, Lee YC, Chen SC. Duodenal-jejunal bypass with sleeve gastrectomy versus the sleeve gastrectomy procedure alone: the role of duodenal exclusion. Surg Obes Relat Dis. 2015; 11:765–770.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Gut Feeling to Cure Diabetes: Potential Mechanisms of Diabetes Remission after Bariatric Surgery
- Meal Management for Patients with Type 2 Diabetes Mellitus Undergoing Metabolic Surgery
- Robotic Roux-en-Y Gastric Bypass and Robotic Sleeve Gastrectomy for Morbid Obesity: Case Reports
- Laparoscopic Hiatal Hernia Repair during Laparoscopic Roux-en-Y Gastric Bypass (LRYGB)
- Initial Experience with Laparoscopic Loop Duodenojejunal Bypass with Sleeve Gastrectomy in Korean Obese Patients
