J Rheum Dis.
2011 Jun;18(2):122-124.
A Case of Arthritis due to Mycobacterium Intracellulare in a Immunocompetent Patient
- Affiliations
-
- 1Department of Internal Medicine, Gangneung Asan Hospital, University of Ulsan College of Medicine, Gangneung, Korea. drkiss@korea.com
- 2Department of Orthopedics, Gangneung Asan Hospital, University of Ulsan College of Medicine, Gangneung, Korea.
Abstract
- Nontuberculous mycobacteria (NTM) are widely distributed in nature and are usually of low pathogenic potential. NTM rarely has been recognized as a cause of musculoskeletal infections that involve joints, bone and soft tissue in immunocompetent patients. The risk factors of its infection are local traumas caused by surgery, injury, or injection. A fifty five-year-old immunocompetent patient visted to hospital due to right wrist mass and pain. Excisional biopsy was done. Histologically granulomatous inflammation was identified and Mycobacterium intracellulare was cultured. Although very rare, NTM should be suspected at least once as a causative pathogen of chronic arthritis when the cause is uncertain.
MeSH Terms
Figure
-
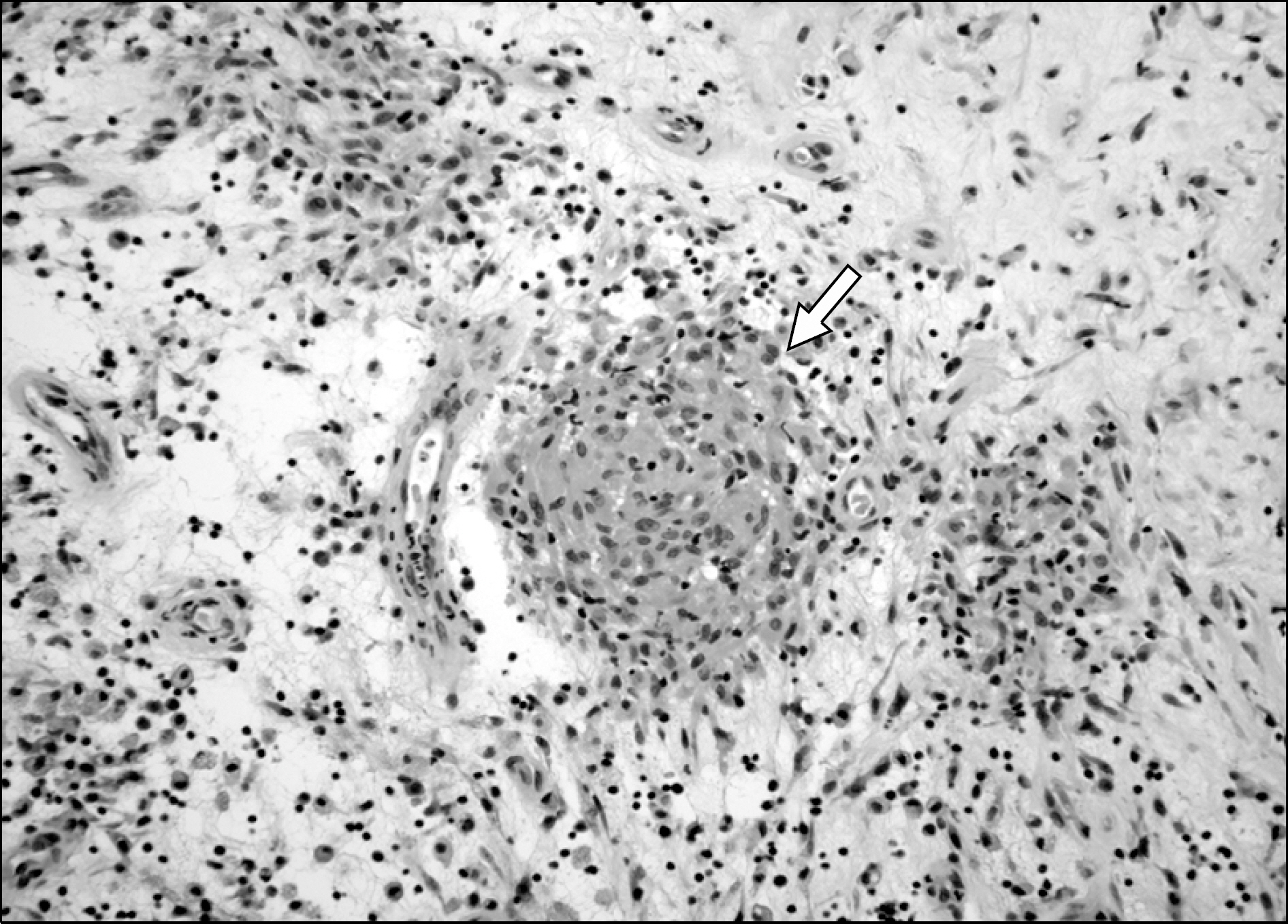
Figure 1. Histologic examination of synovial tissue. Chronic inflammation with histiocytic and epithelioid aggregation (granu-loma) (arrow) is shown (H&E, ×200).

Figure 2. Radiograph in oblique projection of right wrist reveals multiple bone erosions in the distal radius, ular (arrows) and carpal bone (arrowheads).
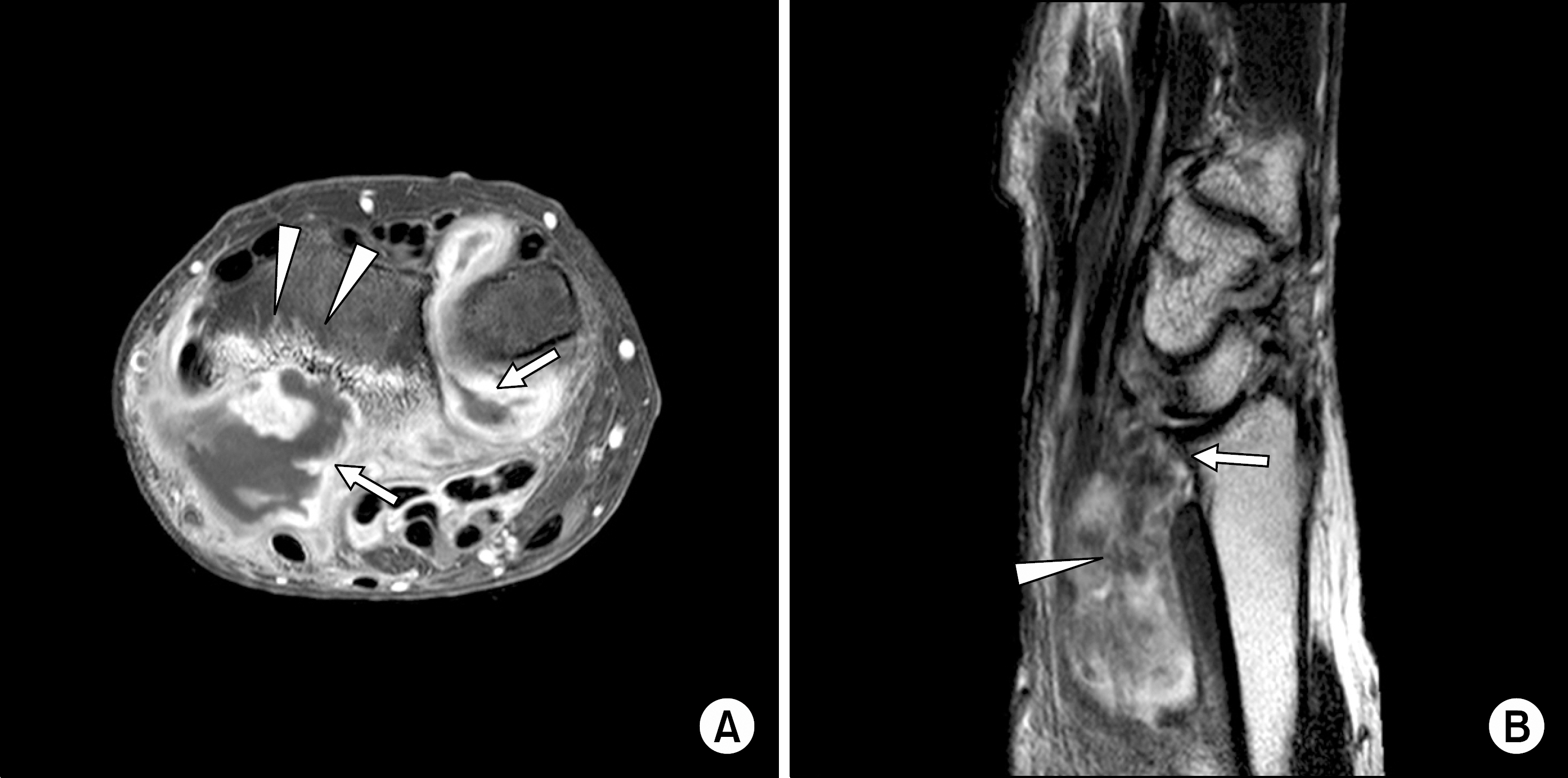
Figure 3. (A) Axial gadolinium- enhanced T1-weighted MR image shows synovial proliferation (arr-ows), bone erosion and bone marrow edema (arrowheads), (B) Sagittal T2-weighted MR image shows radius bone erosion (arrow) and soft tissue mass (arrowhead).
Reference
-
References
1. Kozin SH, Bishop AT. Atypical Mycobacterium infections of the upper extremity. J Hand Surg Am. 1994; 19:480–7.
Article2. Toussirot E, Chevrolet A, Wendling D. Tenosinovitis due to Mycobacterium avium intracellulare and Mycobacterium chelonei: report of two cases with review of the literature. Clin Rheumatol. 1998; 17:152–6.3. Falkinham JO 3rd. Epidemiology of infection by nontuberculous mycobacteria. Clin Microbiol Rev. 1996; 9:177–215.
Article4. Jogi R, Tyring SK. Therapy of nontuberculous mycobacterial infections. Dermatol Ther. 2004; 17:491–8.
Article5. American Thoracic Society. Diagnosis and treatment of disease caused by nontuberculous mycovacteria. Am J Respir Crit Care Med. 1997; 156:S1–S25.6. Park KW, Kwon HH, Chung SH, Kim KC, Choe JY, Lee YH. A Case of Tenosynovitis Due to Mycobacterium intracellulare in a Patient with Rheumatoid Arthritis. Infect Chemother. 2007; 39:59–62.7. Hellinger WC, Smilack JD, Greider JL Jr, Alvarez S, Trigg SD, Brewer NS, et al. Localized soft-tissue infections with Mycobacterium avium/Mycobacterium intracellulare complex in immunocompetent patients: granulomatous tenosynovitis of the hand or wrist. Clin Infect Dis. 1995; 21:65–9.
Article8. Zenone T, Boibieux A, Tigaud S, Fredenucci JF, Vin-cent V, Chidiac C, et al. Non-tuberculous mycobacterial tenosynovitis: a review. Scand J Infect Dis. 1999; 31:221–8.9. Benson CA, Williams PL, Currier JS, Holland F, Mahon LF, MacGregor RR, et al. AIDS Clinical Trials Group 223 Protocol Team. A prospective, randomized trial ex-amining the efficacy and safety of clarithromycin in combination with ethambutol, rifabutin, or both for the treatment of disseminated Mycobacterium avium complex disease in persons with acquired immunodeficiency syndrome. Clin Infect Dis. 2003; 37:1234–43.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Vertebral Osteomyelitis due to Mycobacterium intracellulare in an Immunocompetent Elderly Patient After Vertebroplasty
- A Case of Chronic Arthritis Due to Mycobacterium intracellulare after Trauma
- A Case of Disseminated Mycobacterium intracellulare Infection in an Immunocompromised Host
- Disseminated Mycobacterium intracellulare Infection in an Immunocompetent Host
- A Case of Pulmonary Disease due to Mycobacterium avium-intracellulare complex
