Early Presentation of Heterotopic Ossification Mimicking Pyomyositis: Two Case Reports
- Affiliations
-
- 1Department of Rehabilitation Medicine, Seoul National University College of Medicine, Seoul National University Bundang Hospital, Seongnam 463-707, Korea. drlim1@snu.ac.kr
- 2Department of Rehabilitation Medicine, Armed Forces Capital Hospital, Seongnam 463-040, Korea.
Abstract
- Early diagnosis and treatment of heterotopic ossification (HO) is essential to the prevention of complications. It is difficult to diagnose HO in its initial phase because non-specific clinical manifestations, laboratory findings and imaging findings of immature HO may mimic other diseases such as cellulitis, osteomyelitis, thrombophlebitis, deep vein thrombosis and local infection with abscess. We experienced two cases of HO, which were misdiagnosed as pyomyositis at first by clinical signs and MRI findings indicating the deep infection; the extensive intramuscular ossification appeared later on. We observed an increase of C-reactive protein and creatine kinase followed by the elevation of alkaline phosphatase with abnormal triphasic bone scan. The trajectory of these biomarkers was analyzed to get more insight into the early stages of HO along with the imaging findings. Although our cases cannot be generalized as typical of immature HO, they clearly demonstrate that the change of specific biomarkers with a careful history taking and physical examination should be noted to detect HO as early as possible while avoiding confusion with other mimicking conditions.
Keyword
MeSH Terms
Figure
-

Fig. 1 Changes in x-ray images in a 50-year-old tetraplegic man who had a heterotopic ossification after spinal cord injury; (A) Initial x-ray does not show any definite abnormal findings. (B) Periarticular calcifications are observed around both proximal femurs especially around right lesser trochanteric area (arrowheads). (C) Follow-up X-ray performed one month later shows increased calcifications (arrowheads).

Fig. 2 MRI findings in a 50-year-old tetraplegic man who had a heterotopic ossification after spinal cord injury; Axial (A) and Coronal (B) T2-weighted MR images display hyperintense swelling of muscles (thin arrows) and diffusely increased signal intensity in both buttocks and proximal thighs affecting both iliopsoas, vastus, gluteus and adductor muscle groups (thick arrows). Diffusely increased thickness and signal intensity in the subcutaneous tissues are noted (arrowheads). Coronal (C), axial (D) and sagittal (E) gadolinum-enhanced T1-weighted with fat saturation MR images show heterogenous and feather-like enhancement of the affected muscles such as gluteus maximus, vastus lateralis, vastus medialis and iliopsoas (thin arrows). Also, it reveals intramuscular fluid collections with hypointensity with peripheral rim enhancement (thick arrows).
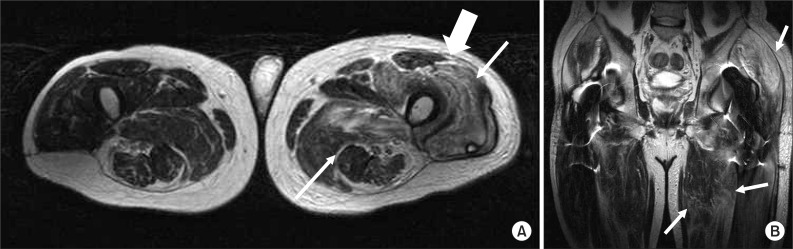
Fig. 3 MRI findings in a 55-year-old man who had a heterotopic ossification after operation for intertrochanteric fracture of left femur; (A) Axial T2-weighted non-enhanced MR image shows diffusely increased signal intensity in left hip muscles (thin arrows) and hyperintense signal along the fascia (thick arrow). (B) Coronal T2-weighted non-enhanced MR image reveals hyperintense infiltration in hip girdle muscles (thin arrows).

Fig. 4 Chronologic changes in the levels of parameters in Case 1 (A) and Case 2 (B). (A) Serum CRP and CK levels increased ahead of the development of swelling followed by the change of serum ALP after confirmation of heterotopic ossification radiographically. (B) CK level was not checked frequently to make the trajectory for its change, but we can notice the increase of CRP and CK followed by the elevation ALP after confirmation of heterotopic ossification radiographically.
Reference
-
1. Shehab D, Elgazzar AH, Collier BD. Heterotopic ossification. J Nucl Med. 2002; 43:346–353. PMID: 11884494.2. Shirkhoda A, Armin AR, Bis KG, Makris J, Irwin RB, Shetty AN. MR imaging of myositis ossificans: variable patterns at different stages. J Magn Reson Imaging. 1995; 5:287–292. PMID: 7633105.
Article3. Singh RS, Craig MC, Katholi CR, Jackson AB, Mountz JM. The predictive value of creatine phosphokinase and alkaline phosphatase in identification of heterotopic ossification in patients after spinal cord injury. Arch Phys Med Rehabil. 2003; 84:1584–1588. PMID: 14639555.4. Taly AB, Nair KP, Jayakumar PN, Ravishankar D, Kalaivani PL, Indiradevi B, Murali T. Neurogenic heterotopic ossification: a diagnostic and therapeutic challenge in neurorehabilitation. Neurol India. 2001; 49:37–40. PMID: 11303239.5. McCarthy EF, Sundaram M. Heterotopic ossification: a review. Skeletal Radiol. 2005; 34:609–619. PMID: 16132978.
Article6. Al-Najar M, Obeidat F, Ajlouni J, Mithqal A, Hadidy A. Primary extensive pyomyositis in an immunocompetent patient: case report and literature review. Clin Rheumatol. 2010; 29:1469–1472. PMID: 20857159.
Article7. Sherman AL, Williams J, Patrick L, Banovac K. The value of serum creatine kinase in early diagnosis of heterotopic ossification. J Spinal Cord Med. 2003; 26:227–230. PMID: 14997963.
Article8. Wick L, Berger M, Knecht H, Glucker T, Ledermann HP. Magnetic resonance signal alterations in the acute onset of heterotopic ossification in patients with spinal cord injury. Eur Radiol. 2005; 15:1867–1875. PMID: 15856244.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Osteomyelitis in Heterotopic Ossification after Trochanteric Pressure Sore Reconstruction: A Case Report
- Heterotopic Ossification of a Partially Ruptured Achilles Tendon (A Case Report)
- Heterotopic Ossification Mimics Neurogenic Tumor: A Case Report
- Heterotopic Ossification of the Elbow after Medial Epicondylectomy
- Heterotopic Ossification Combined with Infection in the Hand: A Case Report
