A case of bisphosphonate-related osteonecrosis of the jaw with a particularly unfavourable course: a case report
- Affiliations
-
- 1Department of Medical Biotechnologies, Dentistry Clinic, University of Siena, Siena, Italy.
- 2Department of Medicine, Surgery and Neurosciences, ENT Clinic, University of Siena, Siena, Italy. mailarticoli@libero.it
- KMID: 2391359
- DOI: http://doi.org/10.5125/jkaoms.2017.43.4.272
Abstract
- Bisphosphonates are drugs used to treat osteoclast-mediated bone resorption, including osteoporosis, Paget disease, multiple myeloma, cancer-related osteolysis, and malignant hypercalcemia. The use of these drugs has increased in recent years as have their complications, especially bisphosphonate-related osteonecrosis of the jaw (BRONJ), which more frequently affects the mandible. Here we report a case of BRONJ with a particularly unfavorable course due to cervical inflammation that developed into necrotizing fasciitis, followed by multiorgan involvement leading to septic shock and death.
Keyword
MeSH Terms
Figure
-

Fig. 1 Panoramic radiograph. Radiologic image shows a fullthickness right jaw fracture.

Fig. 2 Computed tomography scan of the head; coronal view. Coronal view shows biphosphonate-related osteonecrosis lesions, fracture of right jaw and thickening of the soft tissue adjacent the inferior right hemimandibular surface in a 69-year-old woman with breast cancer history and treated with zoledronic acid for 23 administrations.
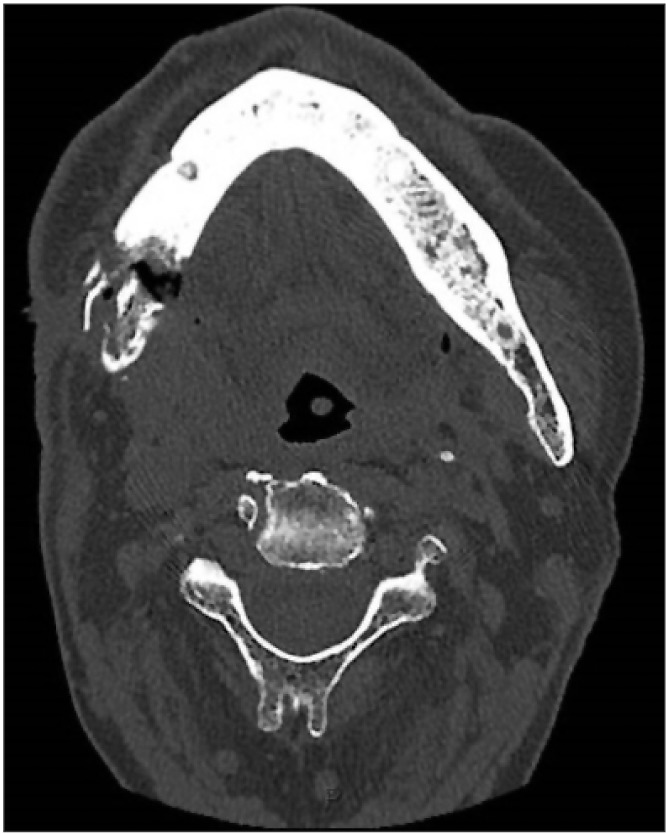
Fig. 3 Computed tomography (CT) scan of the head; transversal view. CT scan of the face, neck and chest was performed without contrast, showing pathological fracture of right jaw and periosteal reaction, besides mixed lytic and sclerotic lesion of the jaw.
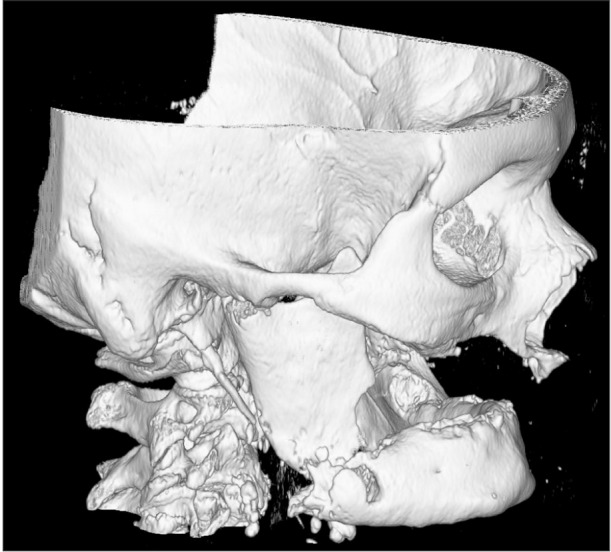
Fig. 4 Three-dimensional computed tomography reconstruction of the head. Radiological image shows a noticeable pathological fracture of right jaw in a 69-year-old woman with breast cancer history and treated with zoledronic acid.
Cited by 1 articles
-
A critical assessment of the medication-related osteonecrosis of the jaw classification in stage I patients: a retrospective analysis
Oliver Ristow, Lena Hürtgen, Julius Moratin, Maximilian Smielowski, Christian Freudlsperger, Michael Engel, Jürgen Hoffmann, Thomas Rückschloß
J Korean Assoc Oral Maxillofac Surg. 2021;47(2):99-111. doi: 10.5125/jkaoms.2021.47.2.99.
Reference
-
1. de Groen PC, Lubbe DF, Hirsch LJ, Daifotis A, Stephenson W, Freedholm D, et al. Esophagitis associated with the use of alendronate. N Engl J Med. 1996; 335:1016–1021. PMID: 8793925.
Article2. Marx RE. Pamidronate (Aredia) and zoledronate (Zometa) induced avascular necrosis of the jaws: a growing epidemic. J Oral Maxillofac Surg. 2003; 61:1115–1117. PMID: 12966493.
Article3. Marx RE, Sawatari Y, Fortin M, Broumand V. Bisphosphonate-induced exposed bone (osteonecrosis/osteopetrosis) of the jaws: risk factors, recognition, prevention, and treatment. J Oral Maxillofac Surg. 2005; 63:1567–1575. PMID: 16243172.
Article4. Woo SB, Hellstein JW, Kalmar JR. Narrative [corrected] review: bisphosphonates and osteonecrosis of the jaws. Ann Intern Med. 2006; 144:753–761. PMID: 16702591.5. Otto S, Schreyer C, Hafner S, Mast G, Ehrenfeld M, Stürzenbaum S, et al. Bisphosphonate-related osteonecrosis of the jaws: characteristics, risk factors, clinical features, localization and impact on oncological treatment. J Craniomaxillofac Surg. 2012; 40:303–309. PMID: 21676622.6. Lee SH, Chan RC, Chang SS, Tan YL, Chang KH, Lee MC, et al. Use of bisphosphonates and the risk of osteonecrosis among cancer patients: a systemic review and meta-analysis of the observational studies. Support Care Cancer. 2014; 22:553–560. PMID: 24203085.
Article7. Ruggiero SL, Woo SB. Biophosphonate-related osteonecrosis of the jaws. Dent Clin North Am. 2008; 52:111–128. ixPMID: 18154867.
Article8. Tsitsilonis S, Druschel C, Wichlas F, Haas NP, Schwabe P, Bail HJ, et al. Necrotizing fasciitis: is the bacterial spectrum changing? Langenbecks Arch Surg. 2013; 398:153–159. PMID: 22833058.
Article9. Greinwald JH Jr, Wilson JF, Haggerty PG. Peritonsillar abscess: an unlikely cause of necrotizing fasciitis. Ann Otol Rhinol Laryngol. 1995; 104:133–137. PMID: 7857015.
Article10. Tung-Yiu W, Jehn-Shyun H, Ching-Hung C, Hung-An C. Cervical necrotizing fasciitis of odontogenic origin: a report of 11 cases. J Oral Maxillofac Surg. 2000; 58:1347–1352. PMID: 11117681.
Article11. Lorenzini G, Picciotti M, Di Vece L, Pepponi E, Brindisi L, Vessio V, et al. Cervical necrotizing fasciitis of odontogenic origin involving the temporal region--a case report. J Craniomaxillofac Surg. 2011; 39:570–573. PMID: 22036666.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Sinusitis due to Bisphosphonate Related Osteonecrosis of Jaw
- Bisphosphonate-Related Osteonecrosis in a Patient with Florid Cemento-Osseous Dysplasia
- Dental implant treatment after healing of bisphosphonate-related osteonecrosis of the jaw (BRONJ) in the same region: a case report
- Bisphosphonate Related Osteonecrosis of the Jaw (BRONJ): Position Statement of Korea
- Clinical feature and treatment of bisphosphonate-related osteonecrosis of jaw about oral bisphosphonate administrated patients: case reports
