Korean J Gastroenterol.
2017 Jul;70(1):4-12. 10.4166/kjg.2017.70.1.4.
The Effect of Hâ‚‚ Receptor Antagonist in Acid Inhibition and Its Clinical Efficacy
- Affiliations
-
- 1Department of Internal Medicine, Seoul National University Bundang Hospital, Seoungnam, Korea. nayoungkim49@empas.com
- 2Department of Internal Medicine and Liver Research Institute, Seoul National University College of Medicine, Seoul, Korea.
- KMID: 2390778
- DOI: http://doi.org/10.4166/kjg.2017.70.1.4
Abstract
- The first histamine Hâ‚‚ receptor antagonists (Hâ‚‚RAs) were developed in the early 1970s. They played a dominant role in treating peptic ulcer disease and gastroesophageal reflux disease (GERD). Hâ‚‚RAs block the production of acid by Hâº, Kâº-ATPase at the parietal cells and produce gastric luminal anacidity for varying periods. Hâ‚‚RAs are highly selective, and they do not affect Hâ‚ receptors. Moreover, they are not anticholinergic agents. Sequential development of Hâ‚‚RAs, proton pump inhibitors (PPIs), and discovery of Helicobacter pylori infection changed the paradigm of peptic ulcer disease with marked decrease of morbidity and mortality. PPIs are known to be the most effective drugs that are currently available for suppressing gastric acid secretion. Many studies have shown its superiority over Hâ‚‚RAs as a treatment for acid-related disorders, such as peptic ulcer disease, GERD, and Zollinger-Ellison syndrome. However, other studies have reported that PPIs may not be able to render stomach achlorhydric and have identified a phenomenon of increasing gastric acidity at night in individuals receiving a PPI twice daily. These nocturnal acid breakthrough episodes can be eliminated with an addition of Hâ‚‚RAs at night. The effectiveness of nighttime dose of Hâ‚‚RA suggests a major role of histamine in nocturnal acid secretion. Hâ‚‚RAs reduce secretion of gastric acid, and each Hâ‚‚RA also has specific effects. For instance, nizitidine alleviates not only symptoms of GERD, but also provokes gastric emptying, resulting in clinical symptom improvement of functional dyspepsia. The aim of this paper was to review the characteristics and role of Hâ‚‚RAs and assess the future strategy and treatment of upper gastrointestinal disease, including acid related disorders.
MeSH Terms
-
Cholinergic Antagonists
Dyspepsia
Gastric Acid
Gastric Emptying
Gastroesophageal Reflux
Gastrointestinal Diseases
Helicobacter pylori
Histamine
Mortality
Peptic Ulcer
Phenobarbital
Proton Pump Inhibitors
Rabeprazole
Stomach
Treatment Outcome*
Zollinger-Ellison Syndrome
Cholinergic Antagonists
Histamine
Phenobarbital
Proton Pump Inhibitors
Figure
-

Fig. 1. A model structure of gastric H+, K+-ATPase. The gastric H+, K+-ATPase α subunit has 3 lobes, N (ATP binding), P (phosphorylation), and A (activation) domains in the cytoplasmic domain, and 3 transmembrane segments in the membrane domain. The gastric β-subunit has a short cytoplasmic region, 1 transmembrane segment, and a heavily glycosylated extracellular region. The number of Asn sites having carbohydrates is based on pig H+, K+-ATPase, as previously described by Shin and Kim.24
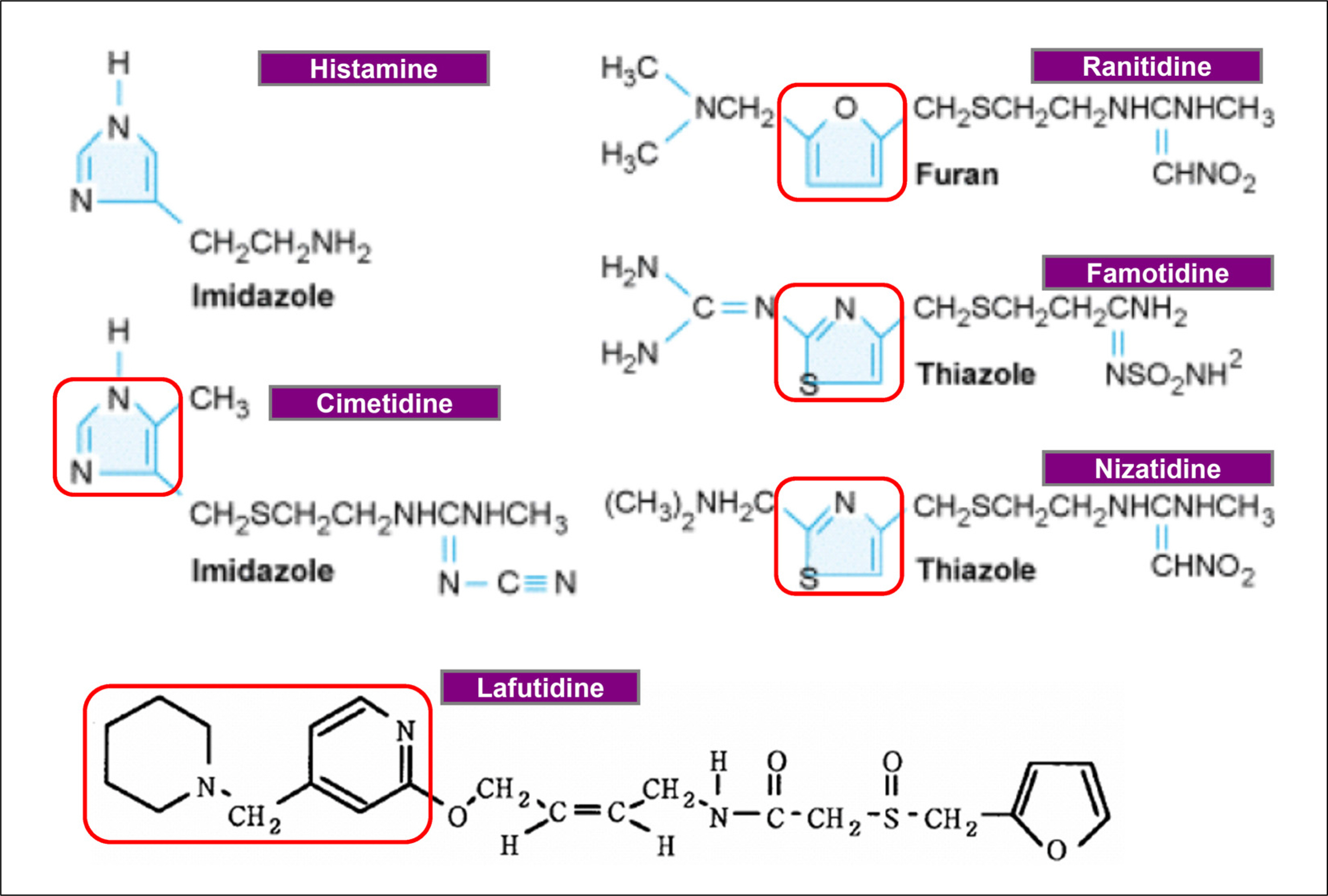
Fig. 2. Structures of H2 receptor antagonists. Red box indicates pyridine ring or modified structures.29–31
Reference
-
References
1. Pounder R. Histamine H2-receptor antagonists. Baillieres Clin Gastroenterol. 1988; 2:593–608.
Article2. Shim YK, Kim N. Nonsteroidal anti-inflammatory drug and aspirin-induced peptic ulcer disease. Korean J Gastroenterol. 2016; 67:300–312.
Article3. Brunner G, Creutzfeldt W, Harke U, Lamberts R. Therapy with omeprazole in patients with peptic ulcerations resistant to extended high-dose ranitidine treatment. Digestion. 1988; 39:80–90.
Article4. Double blind comparative study of omeprazole and ranitidine in patients with duodenal or gastric ulcer: a multicentre trial. Cooperative study group. Gut. 1990; 31:653–656.5. Yeomans ND. New data on healing of nonsteroidal anti-inflammatory drug-associated ulcers and erosions. Omeprazole NSAID Steering Committee. Am J Med. 1998; 104(3A):56S–61S. discussion 79S–80S.6. Lagergren J, Bergström R, Lindgren A, Nyrén O. Symptomatic gastroesophageal reflux as a risk factor for esophageal adenocarcinoma. N Engl J Med. 1999; 340:825–831.
Article7. Katz PO. Pathogenesis and management of gastroesophageal reflux disease. J Clin Gastroenterol. 1991; 13(Suppl 2):S6–S15.
Article8. Fass R, Ofman JJ, Gralnek IM, et al. Clinical and economic assessment of the omeprazole test in patients with symptoms suggestive of gastroesophageal reflux disease. Arch Intern Med. 1999; 159:2161–2168.
Article9. Habu Y, Oyasu K, Wakamatsu T, et al. Cost-effectiveness of the treatment of reflux esophagitis: proton pump inhibitor versus his-tamine-2-receptor antagonist. Nihon Rinsho. 2000; 58:1881–1885.10. Delchier JC, Soule JC, Mignon M, et al. Effectiveness of omeprazole in seven patients with zollinger-ellison syndrome resistant to histamine H2-receptor antagonists. Dig Dis Sci. 1986; 31:693–699.
Article11. Lamers CB, Lind T, Moberg S, Jansen JB, Olbe L. Omeprazole in zollinger-ellison syndrome. Effects of a single dose and of longterm treatment in patients resistant to histamine H2-receptor antagonists. N Engl J Med. 1984; 310:758–761.12. Ducrotté P, Guillemot F, Elouaer-Blanc L, et al. Comparison of omeprazole and famotidine on esophageal pH in patients with moderate to severe esophagitis: a crossover study. Am J Gastroenterol. 1994; 89:717–721.13. Bate CM, Keeling PW, O'Morain C, et al. Comparison of omeprazole and cimetidine in reflux oesophagitis: symptomatic, endoscopic, and histological evaluations. Gut. 1990; 31:968–972.
Article14. Dam G, Vilstrup H, Watson H, Jepsen P. Proton pump inhibitors as a risk factor for hepatic encephalopathy and spontaneous bacterial peritonitis in patients with cirrhosis with ascites. Hepatology. 2016; 64:1265–1272.
Article15. Freedberg DE, Kim LS, Yang YX. The risks and benefits of long-term use of proton pump inhibitors: expert review and best practice advice from the American Gastroenterological Association. Gastroenterology. 2017; 152:706–715.
Article16. Li H, Meng L, Liu F, Wei JF, Wang YQ. H+/K+-ATPase inhibitors: a patent review. Expert Opin Ther Pat. 2013; 23:99–111.
Article17. Andersson K, Carlsson E. Potassium-competitive acid blockade: a new therapeutic strategy in acid-related diseases. Pharmacol Ther. 2005; 108:294–307.
Article18. Hallenbeck GA. What is the best elective operation for duodenal ulcer? Can Med Assoc J. 1970; 103:1255–1262.19. Luff AP. Collective investigation into the after-history of gastroenterostomy. Br Med J. 1930; 1:348–354.
Article20. Kemp D. An evaluation and comparison of the early and late results of standardized polya gastrectomy. Gut. 1967; 8:151–165.
Article21. Whittaker LD Jr, Judd ES, Stauffer MH. Analysis of use of vagotomy with drainage procedure in surgical management of duodenal ulcer. Surg Gynecol Obstet. 1967; 125:1018–1026.22. Kang JM, Seo PJ, Kim N, et al. Analysis of direct medical care costs of peptic ulcer disease in a Korean tertiary medical center. Scand J Gastroenterol. 2012; 47:36–42.
Article23. Sachs G, Chang HH, Rabon E, Schackman R, Lewin M, Saccomani G. A nonelectrogenic H+ pump in plasma membranes of hog stomach. J Biol Chem. 1976; 251:7690–7698.
Article24. Shin JM, Kim N. Pharmacokinetics and pharmacodynamics of the proton pump inhibitors. J Neurogastroenterol Motil. 2013; 19:25–35.
Article25. Black JW, Duncan WA, Durant CJ, Ganellin CR, Parsons EM. Definition and antagonism of histamine H 2-receptors. Nature. 1972; 236:385–390.26. Okabe S, Takeuchi K, Urushidani T, Takagi K. Effects of cimetidine, a histamine H2-receptor antagonist, on various experimental gastric and duodenal ulcers. Am J Dig Dis. 1977; 22:677–684.
Article27. Macdougall BR, Bailey RJ, Williams R. H2-receptor antagonists and antacids in the prevention of acute gastrointestinal haemorrhage in fulminant hepatic failure. Two controlled trials. Lancet. 1977; 1:617–619.28. Jones RH, Rudge CJ, Bewick M, Parsons V, Weston MJ. Cimetidine: prophylaxis against upper gastrointestinal haemorrhage after renal transplantation. Br Med J. 1978; 1:398–400.
Article29. Bossi A, Romeo G, Pezzoli A. Side-effects, structure, and H2-receptor antagonists. Lancet. 1992; 339:1366.
Article30. Song WJ, Kim MH, Lee SM, et al. Two cases of h(2)-receptor antagonist hypersensitivity and cross-reactivity. Allergy Asthma Immunol Res. 2011; 3:128–131.
Article31. Aihara T, Nakamura E, Amagase K, et al. Pharmacological control of gastric acid secretion for the treatment of acid-related peptic disease: past, present, and future. Pharmacol Ther. 2003; 98:109–127.
Article32. Berardi RR, Tankanow RM, Nostrant TT. Comparison of famotidine with cimetidine and ranitidine. Clin Pharm. 1988; 7:271–284.33. Frank WO, Young M, Palmer RH, Karlstadt R, Rockhold F, Mounce W. Once-daily bedtime dosing regimen of cimetidine in the treatment of gastric ulcer. Clin Ther. 1988; 11:595–603.34. Weir DG. Peptic ulceration. Br Med J (Clin Res Ed). 1988; 296:195–200.35. Wilder-Smith CH, Ernst T, Gennoni M, Zeyen B, Halter F, Merki HS. Tolerance to oral H2-receptor antagonists. Dig Dis Sci. 1990; 35:976–983.
Article36. Fullarton GM, McLauchlan G, Macdonald A, Crean GP, McColl KE. Rebound nocturnal hypersecretion after four weeks treatment with an H2 receptor antagonist. Gut. 1989; 30:449–454.
Article37. Nwokolo CU, Smith JT, Gavey C, Sawyerr A, Pounder RE. Tolerance during 29 days of conventional dosing with cimetidine, nizatidine, famotidine or ranitidine. Aliment Pharmacol Ther. 1989; 4(Suppl 1):29–45.38. Komazawa Y, Adachi K, Mihara T, et al. Tolerance to famotidine and ranitidine treatment after 14 days of administration in healthy subjects without helicobacter pylori infection. J Gastroenterol Hepatol. 2003; 18:678–682.39. Adachi K, Fujishiro H, Katsube T, et al. Predominant nocturnal acid reflux in patients with Los Angeles grade C and D reflux esophagitis. J Gastroenterol Hepatol. 2001; 16:1191–1196.
Article40. Festen HP, Schenk E, Tan G, Snel P, Nelis F. Omeprazole versus high-dose ranitidine in mild gastroesophageal reflux disease: short-and long-term treatment. The Dutch Reflux Study Group. Am J Gastroenterol. 1999; 94:931–936.41. Katsube T, Adachi K, Kawamura A, et al. Helicobacter pylori infection influences nocturnal gastric acid breakthrough. Aliment Pharmacol Ther. 2000; 14:1049–1056.
Article42. Bezwoda W, Charlton R, Bothwell T, Torrance J, Mayet F. The importance of gastric hydrochloric acid in the absorption of non-heme food iron. J Lab Clin Med. 1978; 92:108–116.43. Golubov J, Flanagan P, Adams P. Inhibition of iron absorption by omeprazole in rat model. Dig Dis Sci. 1991; 36:405–408.
Article44. Wallace JL, Sharkey KA. Pharmacotherapy of gastric acidity, peptic ulcers and gastroesophageal reflux disease. Brunton LL, Chabner BA, Knollmann BC, editors. Goodman & Gilman's the pharmacological basis of therapeutics. 12th ed.New York: McGraw-Hill Education;2011. p. 1309–1322.45. Qadeer MA, Richter JE, Brotman DJ. Hospital‐acquired gastrointestinal bleeding outside the critical care unit: risk factors, role of acid suppression, and endoscopy findings. J Hosp Med. 2006; 1:13–20.
Article46. Leite LP, Johnston BT, Just RJ, Castell DO. Persistent acid secretion during omeprazole therapy: a study of gastric acid profiles in patients demonstrating failure of omeprazole therapy. Am J Gastroenterol. 1996; 91:1527–1531.47. Kuo B, Castell DO. Optimal dosing of omeprazole 40 mg daily: effects on gastric and esophageal pH and serum gastrin in healthy controls. Am J Gastroenterol. 1996; 91:1532–1538.48. Peghini PL, Katz PO, Bracy NA, Castell DO. Nocturnal recovery of gastric acid secretion with twice-daily dosing of proton pump inhibitors. Am J Gastroenterol. 1998; 93:763–767.
Article49. Katz PO, Anderson C, Khoury R, Castell DO. Gastro-oesophageal reflux associated with nocturnal gastric acid breakthrough on proton pump inhibitors. Aliment Pharmacol Ther. 1998; 12:1231–1234.
Article50. Fackler WK, Vaezi MF, Ours TM, Richter JE. Nocturnal acid breakthrough cannot be eliminated in patients with atypical gastroesophageal reflux disease. Gastroenterology. 2000; 118:A15.
Article51. Peghini PL, Katz PO, Castell DO. Ranitidine controls nocturnal gastric acid breakthrough on omeprazole: a controlled study in normal subjects. Gastroenterology. 1998; 115:1335–1339.
Article52. Walsh JH, Richardson CT, Fordtran JS. pH dependence of acid secretion and gastrin release in normal and ulcer subjects. J Clin Invest. 1975; 55:462–468.
Article53. Lancaster-Smith MJ, Jaderberg ME, Jackson DA. Ranitidine in the treatment of non-steroidal anti-inflammatory drug associated gastric and duodenal ulcers. Gut. 1991; 32:252–255.
Article54. Walan A, Bader JP, Classen M, et al. Effect of omeprazole and ranitidine on ulcer healing and relapse rates in patients with benign gastric ulcer. N Engl J Med. 1989; 320:69–75.
Article55. Soll AH, Achord JL, Bozymski G, et al. Medical treatment of peptic ulcer disease: practice guidelines. JAMA. 1996; 275:622–629.56. Roth SH, Bennett RE, Mitchell CS, Hartman RJ. Cimetidine therapy in nonsteroidal anti-inflammatory drug gastropathy. Double-blind long-term evaluation. Arch Intern Med. 1987; 147:1798–1801.
Article57. Ehsanullah RS, Page MC, Tildesley G, Wood JR. Prevention of gastroduodenal damage induced by non-steroidal anti-inflammatory drugs: controlled trial of ranitidine. BMJ. 1988; 297:1017–1021.
Article58. Robinson MG, Griffin JW Jr, Bowers J, et al. Effect of ranitidine on gastroduodenal mucosal damage induced by nonsteroidal anti-inflammatory drugs. Dig Dis Sci. 1989; 34:424–428.59. Jones DB, Howden CW, Burget DW, Kerr GD, Hunt RH. Acid suppression in duodenal ulcer: a metaanalysis to define optimal dosing with antisecretory drugs. Gut. 1987; 28:1120–1127.
Article60. Taha AS, Hudson N, Hawkey CJ, et al. Famotidine for the prevention of gastric and duodenal ulcers caused by nonsteroidal antiinflammatory drugs. N Engl J Med. 1996; 334:1435–1439.
Article61. Graham DY, Lidsky MD, Cox AM, et al. Longterm nonsteroidal antiinflammatory drug use and helicobacter pylori infection. Gastroenterology. 1991; 100:1653–1657.
Article62. National institutes of health consensus development conference panel statement: management of hepatitis C. Hepatology. 1997; 26(3 Suppl 1):2S–10S.63. Hudson N, Balsitis M, Filipowicz F, Hawkey CJ. Effect of helicobacter pylori colonisation on gastric mucosal eicosanoid synthesis in patients taking non-steroidal anti-inflammatory drugs. Gut. 1993; 34:748–751.
Article64. Yeomans ND, Tulassay Z, Juhász L, et al. A comparison of omeprazole with ranitidine for ulcers associated with nonsteroidal anti-inflammatory drugs. Acid Suppression Trial: Ranitidine versus Omeprazole for NSAID-associated Ulcer Treatment (ASTRONAUT) Study Group. N Engl J Med. 1998; 338:719–726.65. Kim YS, Kim N, Kim GH. Sex and gender differences in gastroesophageal reflux disease. J Neurogastroenterol Motil. 2016; 22:575–588.
Article66. van Pinxteren B, Numans ME, Bonis PA, Lau J. Short‐term treatment with proton pump inhibitors, H2‐receptor antagonists and prokinetics for gastro‐oesophageal reflux disease‐like symptoms and endoscopy negative reflux disease. Cochrane Database Syst Rev. 2006; (3):CD002095.
Article67. Khan M, Santana J, Donnellan C, Preston C, Moayyedi P. Medical treatments in the short term management of reflux oesophagitis. Cochrane Database Syst Rev. 2007; (2):CD003244.
Article68. Dean BB, Gano AD Jr, Knight K, Ofman JJ, Fass R. Effectiveness of proton pump inhibitors in nonerosive reflux disease. Clin Gastroenterol Hepatol. 2004; 2:656–664.
Article69. Zacny J, Zamakhshary M, Sketris I, Veldhuyzen van Zanten S. Systematic review: the efficacy of intermittent and on‐demand therapy with histamine H2‐receptor antagonists or proton pump inhibitors for gastro‐oesophageal reflux disease patients. Aliment Pharmacol Ther. 2005; 21:1299–1312.
Article70. Fackler WK, Ours TM, Vaezi MF, Richter JE. Longterm effect of H2RA therapy on nocturnal gastric acid breakthrough. Gastroenterology. 2002; 122:625–632.
Article71. Mainie I, Tutuian R, Castell DO. Addition of a H2 receptor antagonist to PPI improves acid control and decreases nocturnal acid breakthrough. J Clin Gastroenterol. 2008; 42:676–679.
Article72. Dodds WJ, Hogan WJ, Helm JF, Dent J. Pathogenesis of reflux esophagitis. Gastroenterology. 1981; 81:376–394.
Article73. Isolauri J, Laippala P. Prevalence of symptoms suggestive of gastroesophageal reflux disease in an adult population. Ann Med. 1995; 27:67–70.
Article74. Vigneri S, Termini R, Leandro G, et al. A comparison of five maintenance therapies for reflux esophagitis. N Engl J Med. 1995; 333:1106–1110.
Article75. Kawano S, Murata H, Tsuji S, et al. Randomized comparative study of omeprazole and famotidine in reflux esophagitis. J Gastroenterol Hepatol. 2002; 17:955–959.
Article76. Neya T, Itano N, Mizutani M, Yamasato T, Takaki M, Nakayama S. The effect of cisapride on neural 5-HT receptors in guinea-pig isolated ileum. Eur J Pharmacol. 1984; 106:221–222.
Article77. Ueki S, Matsunaga Y, Yoneta T, Tamaki H, Itoh Z. Gastroprokinetic activity of nizatidine during the digestive state in the dog and rat. Arzneimittelforschung. 1999; 49:618–625.
Article78. Futagami S, Shimpuku M, Song JM, et al. Nizatidine improves clinical symptoms and gastric emptying in patients with functional dyspepsia accompanied by impaired gastric emptying. Digestion. 2012; 86:114–121.
Article79. Inauen W, Emde C, Weber B, et al. Effects of ranitidine and cisapride on acid reflux and oesophageal motility in patients with reflux oesophagitis: a 24 hour ambulatory combined pH and manometry study. Gut. 1993; 34:1025–1031.
Article80. Sekiguchi T, Nishioka T, Matsuzaki T, et al. Comparative efficacy of acid reflux inhibition by drug therapy in reflux esophagitis. Gastroenterol Jpn. 1991; 26:137–144.
Article81. Adachi K, Ono M, Kawamura A, Yuki M, Fujishiro H, Kinoshita Y. Nizatidine and cisapride enhance salivary secretion in humans. Aliment Pharmacol Ther. 2002; 16:297–301.
Article82. Adachi K, Furuta K, Katsube T, et al. Nizatidine and cisapride increase salivary secretion in rats. Dig Dis Sci. 2004; 49:399–403.
Article83. Sonnenberg A, Steinkamp U, Weise A, et al. Salivary secretion in reflux esophagitis. Gastroenterology. 1982; 83:889–895.
Article84. Helm JF, Dodds WJ, Hogan WJ, Soergel KH, Egide MS, Wood CM. Acid neutralizing capacity of human saliva. Gastroenterology. 1982; 83(1 Pt 1):69–74.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Advances in the management of diabetic kidney disease: beyond sodium-glucose co-transporter 2 inhibitors
- Effect of GABA on the contratility of small intestine isolated from rat
- Antagonists of NMDA Receptor, Calcium Channel and Protein Kinase C Potentiate Inhibitory Action of Morphine on Responses of Rat Dorsal Horn Neuron
- Effect of diazepam on the oxytocin induced contraction of the isolated rat uterus
- Rapid-Acting Antidepressant Effect of Ketamine and Its Clinical Application
