CTNNB1 Mutation in Aldosterone Producing Adenoma
- Affiliations
-
- 1Division of Nephrology, Department of Internal Medicine, Chi Mei Medical Center, Liouying, Tainan City, Taiwan.
- 2TAIPAI (Taiwan Primary Aldosteronism investigator), Taipei, Taiwan. q91421028@ntu.edu.tw
- 3Division of Nephrology, Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan.
- 4Division of Endocrinology and Metabolism, Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan.
- KMID: 2389813
- DOI: http://doi.org/10.3803/EnM.2017.32.3.332
Abstract
- Discoveries of somatic mutations permit the recognition of subtypes of aldosterone-producing adenomas (APAs) with distinct clinical presentations and pathological features. Catenin β1 (CTNNB1) mutation in APAs has been recently described and discussed in the literature. However, significant knowledge gaps still remain regarding the prevalence, clinical characteristics, pathophysiology, and outcomes in APA patients harboring CTNNB1 mutations. Aberrant activation of the Wnt/β-catenin signaling pathway will further modulate tumorigenesis. We also discuss the recent knowledge of CTNNB1 mutation in adrenal adenomas.
Keyword
Figure
-
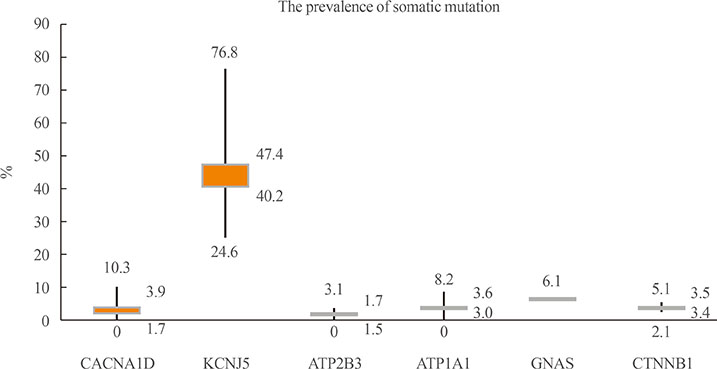
Fig. 1 The prevalence of the most known mutation of aldosterone producing adenoma. This box plot displays the full range of variation (from maximum, mean, medium to minimum, accordingly) in each index somatic mutation. CACNA1D, calcium voltage-gated channel subunit α1 D; KCNJ5, potassium voltage-gated channel subfamily J member 5; ATP2B3, ATPase plasma membrane Ca2+ transporting 3; ATP1A1, ATPase Na+/K+ transporting subunit α1; GNAS, guanine nucleotide binding protein, α stimulating; CTNNB1, catenin β1.

Fig. 2 A two-hit model for the pathogenesis of aldosterone-producing adenoma (APA). (A, B) Primary hit: Somatic mutations in CACNA1D, KCNJ5, ATP2B3, ATP1A1, and possibly other genetic alterations produce cell depolarization, increased cytoplasmic calcium level and increased CYP11B2 expression, causing aldosterone hypersecretion. Secondary hit: Aberrant activation of signaling pathways (such as Wnt/β-catenin, Shh, PKA, etc.) causes imbalances between cell proliferation and death in the adrenal, leading to adenoma formation. (A) Adapted from Lalli et al., with permission from Elsevier [36]. (B) Adapted from Seidel et al. [37]. CACNA1D, calcium voltage-gated channel subunit α1 D; KCNJ5, potassium voltage-gated channel subfamily J member 5; ATP2B3, ATPase plasma membrane Ca2+ transporting 3; ATP1A1, ATPase Na+/K+ transporting subunit α1; APCC, aldosterone-producing cell clusters; HSD3b, hydroxy-δ-5-steroid dehydrogenase, 3β- and steroid δ-isomerase cluster; CTNNB1, catenin β1; DACH1, dachshund family transcription factor 1; Shh, sonic hedgehog; PKA, protein kinase A; Ang II, angiotensin II; AT1, Ang II type 1; CAMK, Ca2+/calmodulin-dependent protein kinase; CYP11B2, cytochrome P450 family 11 subfamily B member 2.
Reference
-
1. Mulatero P, Stowasser M, Loh KC, Fardella CE, Gordon RD, Mosso L, et al. Increased diagnosis of primary aldosteronism, including surgically correctable forms, in centers from five continents. J Clin Endocrinol Metab. 2004; 89:1045–1050.2. Fogari R, Preti P, Zoppi A, Rinaldi A, Fogari E, Mugellini A. Prevalence of primary aldosteronism among unselected hypertensive patients: a prospective study based on the use of an aldosterone/renin ratio above 25 as a screening test. Hypertens Res. 2007; 30:111–117.3. Rossi GP, Bernini G, Caliumi C, Desideri G, Fabris B, Ferri C, et al. A prospective study of the prevalence of primary aldosteronism in 1,125 hypertensive patients. J Am Coll Cardiol. 2006; 48:2293–2300.4. Hannemann A, Bidlingmaier M, Friedrich N, Manolopoulou J, Spyroglou A, Volzke H, et al. Screening for primary aldosteronism in hypertensive subjects: results from two German epidemiological studies. Eur J Endocrinol. 2012; 167:7–15.5. Wu VC, Wang SM, Chueh SJ, Yang SY, Huang KH, Lin YH, et al. The prevalence of CTNNB1 mutations in primary aldosteronism and consequences for clinical outcomes. Sci Rep. 2017; 7:39121.6. Wu VC, Huang KH, Peng KY, Tsai YC, Wu CH, Wang SM, et al. Prevalence and clinical correlates of somatic mutation in aldosterone producing adenoma-Taiwanese population. Sci Rep. 2015; 5:11396.7. Zheng FF, Zhu LM, Nie AF, Li XY, Lin JR, Zhang K, et al. Clinical characteristics of somatic mutations in Chinese patients with aldosterone-producing adenoma. Hypertension. 2015; 65:622–628.8. Akerstrom T, Maharjan R, Sven Willenberg H, Cupisti K, Ip J, Moser A, et al. Activating mutations in CTNNB1 in aldosterone producing adenomas. Sci Rep. 2016; 6:19546.9. Xekouki P, Hatch MM, Lin L, Rodrigo de A, Azevedo M, de la Luz Sierra M, et al. KCNJ5 mutations in the National Institutes of Health cohort of patients with primary hyperaldosteronism: an infrequent genetic cause of Conn's syndrome. Endocr Relat Cancer. 2012; 19:255–260.10. Taguchi R, Yamada M, Nakajima Y, Satoh T, Hashimoto K, Shibusawa N, et al. Expression and mutations of KCNJ5 mRNA in Japanese patients with aldosterone-producing adenomas. J Clin Endocrinol Metab. 2012; 97:1311–1319.11. Kitamoto T, Suematsu S, Matsuzawa Y, Saito J, Omura M, Nishikawa T. Comparison of cardiovascular complications in patients with and without KCNJ5 gene mutations harboring aldosterone-producing adenomas. J Atheroscler Thromb. 2015; 22:191–200.12. Boulkroun S, Beuschlein F, Rossi GP, Golib-Dzib JF, Fischer E, Amar L, et al. Prevalence, clinical, and molecular correlates of KCNJ5 mutations in primary aldosteronism. Hypertension. 2012; 59:592–598.13. Azizan EA, Murthy M, Stowasser M, Gordon R, Kowalski B, Xu S, et al. Somatic mutations affecting the selectivity filter of KCNJ5 are frequent in 2 large unselected collections of adrenal aldosteronomas. Hypertension. 2012; 59:587–591.14. Kuppusamy M, Caroccia B, Stindl J, Bandulik S, Lenzini L, Gioco F, et al. A novel KCNJ5-insT149 somatic mutation close to, but outside, the selectivity filter causes resistant hypertension by loss of selectivity for potassium. J Clin Endocrinol Metab. 2014; 99:E1765–E1773.15. Scholl UI, Healy JM, Thiel A, Fonseca AL, Brown TC, Kunstman JW, et al. Novel somatic mutations in primary hyperaldosteronism are related to the clinical, radiological and pathological phenotype. Clin Endocrinol (Oxf). 2015; 83:779–789.16. Scholl UI, Goh G, Stolting G, de Oliveira RC, Choi M, Overton JD, et al. Somatic and germline CACNA1D calcium channel mutations in aldosterone-producing adenomas and primary aldosteronism. Nat Genet. 2013; 45:1050–1054.17. Nakajima Y, Okamura T, Horiguchi K, Gohko T, Miyamoto T, Satoh T, et al. GNAS mutations in adrenal aldosterone-producing adenomas. Endocr J. 2016; 63:199–204.18. Beuschlein F, Boulkroun S, Osswald A, Wieland T, Nielsen HN, Lichtenauer UD, et al. Somatic mutations in ATP1A1 and ATP2B3 lead to aldosterone-producing adenomas and secondary hypertension. Nat Genet. 2013; 45:440–444.19. Williams TA, Monticone S, Schack VR, Stindl J, Burrello J, Buffolo F, et al. Somatic ATP1A1, ATP2B3, and KCNJ5 mutations in aldosterone-producing adenomas. Hypertension. 2014; 63:188–195.20. Akerstrom T, Crona J, Delgado Verdugo A, Starker LF, Cupisti K, Willenberg HS, et al. Comprehensive re-sequencing of adrenal aldosterone producing lesions reveal three somatic mutations near the KCNJ5 potassium channel selectivity filter. PLoS One. 2012; 7:e41926.21. Fernandes-Rosa FL, Williams TA, Riester A, Steichen O, Beuschlein F, Boulkroun S, et al. Genetic spectrum and clinical correlates of somatic mutations in aldosterone-producing adenoma. Hypertension. 2014; 64:354–361.22. Hong AR, Kim JH, Song YS, Lee KE, Seo SH, Seong MW, et al. Genetics of aldosterone-producing adenoma in Korean patients. PLoS One. 2016; 11:e0147590.23. Boulkroun S, Samson-Couterie B, Golib-Dzib JF, Amar L, Plouin PF, Sibony M, et al. Aldosterone-producing adenoma formation in the adrenal cortex involves expression of stem/progenitor cell markers. Endocrinology. 2011; 152:4753–4763.24. Berthon A, Sahut-Barnola I, Lambert-Langlais S, de Joussineau C, Damon-Soubeyrand C, Louiset E, et al. Constitutive beta-catenin activation induces adrenal hyperplasia and promotes adrenal cancer development. Hum Mol Genet. 2010; 19:1561–1576.25. Heikkila M, Peltoketo H, Leppaluoto J, Ilves M, Vuolteenaho O, Vainio S. Wnt-4 deficiency alters mouse adrenal cortex function, reducing aldosterone production. Endocrinology. 2002; 143:4358–4365.26. Kim AC, Reuter AL, Zubair M, Else T, Serecky K, Bingham NC, et al. Targeted disruption of beta-catenin in Sf1-expressing cells impairs development and maintenance of the adrenal cortex. Development. 2008; 135:2593–2602.27. Tissier F, Cavard C, Groussin L, Perlemoine K, Fumey G, Hagnere AM, et al. Mutations of beta-catenin in adrenocortical tumors: activation of the Wnt signaling pathway is a frequent event in both benign and malignant adrenocortical tumors. Cancer Res. 2005; 65:7622–7627.28. Liu C, Li Y, Semenov M, Han C, Baeg GH, Tan Y, et al. Control of beta-catenin phosphorylation/degradation by a dual-kinase mechanism. Cell. 2002; 108:837–847.29. Bjorklund P, Lindberg D, Akerstrom G, Westin G. Stabilizing mutation of CTNNB1/beta-catenin and protein accumulation analyzed in a large series of parathyroid tumors of Swedish patients. Mol Cancer. 2008; 7:53.30. Durand J, Lampron A, Mazzuco TL, Chapman A, Bourdeau I. Characterization of differential gene expression in adrenocortical tumors harboring beta-catenin (CTNNB1) mutations. J Clin Endocrinol Metab. 2011; 96:E1206–E1211.31. Morin PJ, Sparks AB, Korinek V, Barker N, Clevers H, Vogelstein B, et al. Activation of beta-catenin-Tcf signaling in colon cancer by mutations in beta-catenin or APC. Science. 1997; 275:1787–1790.32. Teo AE, Garg S, Shaikh LH, Zhou J, Karet Frankl FE, Gurnell M, et al. Pregnancy, primary aldosteronism, and adrenal CTNNB1 mutations. N Engl J Med. 2015; 373:1429–1436.33. Boulkroun S, Samson-Couterie B, Dzib JF, Lefebvre H, Louiset E, Amar L, et al. Adrenal cortex remodeling and functional zona glomerulosa hyperplasia in primary aldosteronism. Hypertension. 2010; 56:885–892.34. Fernandes-Rosa FL, Giscos-Douriez I, Amar L, Gomez-Sanchez CE, Meatchi T, Boulkroun S, et al. Different somatic mutations in multinodular adrenals with aldosterone-producing adenoma. Hypertension. 2015; 66:1014–1022.35. Dekkers T, ter Meer M, Lenders JW, Hermus AR, Schultze Kool L, Langenhuijsen JF, et al. Adrenal nodularity and somatic mutations in primary aldosteronism: one node is the culprit? J Clin Endocrinol Metab. 2014; 99:E1341–E1351.36. Lalli E, Barhanin J, Zennaro MC, Warth R. Local control of aldosterone production and primary aldosteronism. Trends Endocrinol Metab. 2016; 27:123–131.37. Seidel E, Scholl UI. Intracellular molecular differences in aldosterone: compared to cortisol-secreting adrenal cortical adenomas. Front Endocrinol (Lausanne). 2016; 7:75.38. El Wakil A, Lalli E. The Wnt/beta-catenin pathway in adrenocortical development and cancer. Mol Cell Endocrinol. 2011; 332:32–37.39. Nanba K, Chen AX, Omata K, Vinco M, Giordano TJ, Else T, et al. Molecular heterogeneity in aldosterone-producing adenomas. J Clin Endocrinol Metab. 2016; 101:999–1007.40. Safe S, Kasiappan R. Natural products as mechanism-based anticancer agents: sp transcription factors as targets. Phytother Res. 2016; 30:1723–1732.41. Tadjine M, Lampron A, Ouadi L, Bourdeau I. Frequent mutations of beta-catenin gene in sporadic secreting adrenocortical adenomas. Clin Endocrinol (Oxf). 2008; 68:264–270.42. Heaton JH, Wood MA, Kim AC, Lima LO, Barlaskar FM, Almeida MQ, et al. Progression to adrenocortical tumorigenesis in mice and humans through insulin-like growth factor 2 and β-catenin. Am J Pathol. 2012; 181:1017–1033.43. Phelps RA, Chidester S, Dehghanizadeh S, Phelps J, Sandoval IT, Rai K, et al. A two-step model for colon adenoma initiation and progression caused by APC loss. Cell. 2009; 137:623–634.44. Funder JW, Carey RM, Mantero F, Murad MH, Reincke M, Shibata H, et al. The management of primary aldosteronism: case detection, diagnosis, and treatment: an Endocrine Society Clinical Practice guideline. J Clin Endocrinol Metab. 2016; 101:1889–1916.45. Bonnet S, Gaujoux S, Launay P, Baudry C, Chokri I, Ragazzon B, et al. Wnt/β-catenin pathway activation in adrenocortical adenomas is frequently due to somatic CTNNB1-activating mutations, which are associated with larger and non-secreting tumors: a study in cortisol-secreting and -nonsecreting tumors. J Clin Endocrinol Metab. 2011; 96:E419–E426.46. Gaujoux S, Grabar S, Fassnacht M, Ragazzon B, Launay P, Libe R, et al. β-Catenin activation is associated with specific clinical and pathologic characteristics and a poor outcome in adrenocortical carcinoma. Clin Cancer Res. 2011; 17:328–336.47. Thiel A, Reis AC, Haase M, Goh G, Schott M, Willenberg HS, et al. PRKACA mutations in cortisol-producing adenomas and adrenal hyperplasia: a single-center study of 60 cases. Eur J Endocrinol. 2015; 172:677–685.48. Berthon A, Drelon C, Ragazzon B, Boulkroun S, Tissier F, Amar L, et al. WNT/β-catenin signalling is activated in aldosterone-producing adenomas and controls aldosterone production. Hum Mol Genet. 2014; 23:889–905.49. Pusantisampan T, Sangkhathat S, Kayasut K, Kanngurn S, Jaruratanasirikul S, Chotsampancharoen T, et al. Cushing's syndrome in an infant secondary to malignant adrenocortical tumors with somatic mutation of beta-catenin. Pediatr Dev Pathol. 2010; 13:238–242.50. Cao Y, He M, Gao Z, Peng Y, Li Y, Li L, et al. Activating hotspot L205R mutation in PRKACA and adrenal Cushing's syndrome. Science. 2014; 344:913–917.51. Beuschlein F, Fassnacht M, Assie G, Calebiro D, Stratakis CA, Osswald A, et al. Constitutive activation of PKA catalytic subunit in adrenal Cushing's syndrome. N Engl J Med. 2014; 370:1019–1028.52. Goh G, Scholl UI, Healy JM, Choi M, Prasad ML, Nelson-Williams C, et al. Recurrent activating mutation in PRKACA in cortisol-producing adrenal tumors. Nat Genet. 2014; 46:613–617.53. Sato Y, Maekawa S, Ishii R, Sanada M, Morikawa T, Shiraishi Y, et al. Recurrent somatic mutations underlie corticotropin-independent Cushing's syndrome. Science. 2014; 344:917–920.54. Assie G, Libe R, Espiard S, Rizk-Rabin M, Guimier A, Luscap W, et al. ARMC5 mutations in macronodular adrenal hyperplasia with Cushing's syndrome. N Engl J Med. 2013; 369:2105–2114.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A case of idiopathic hyperaldosteronism vs. bilateral aldosterone producing adenoma
- A Case of Persistent Hyperkalemia After Unilateral Adrenalectomy for Aldosterone-Producing Adenoma
- Anesthetic Experience with Primary Aldosteronism: Report of a case
- Two Case of Primary Aldosteronism Induced by Aldosterone Producing Adrenal Adenoma in a Family
- A Case of a Coexisting Aldosterone-Producing Adrenal Adenoma and Ipsilateral Renal Artery Stenosis
