A Case of Breast Cancer Brain Metastasis with a 16-Year Time Interval without Evidence of Cancer Recurrence
- Affiliations
-
- 1Department of Neurosurgery, Teikyo University Mizonokuchi Hospital, Kawasaki, Japan. merrityamada@hotmail.co.jp
- 2Department of Neurology, Teikyo University Mizonokuchi Hospital, Kawasaki, Japan.
- KMID: 2389761
- DOI: http://doi.org/10.4048/jbc.2017.20.2.212
Abstract
- The median time of brain metastasis from the diagnosis of breast cancer is approximately 3 years. In this case report, a 69-year-old woman demonstrated cerebellar ataxia. Brain magnetic resonance imaging revealed enhanced lesions in bilateral cerebellar hemispheres. She had undergone surgery, radiation, and chemotherapy for uterine and breast cancer 24 years prior and 16 years prior, respectively. Although she had not received any anticancer treatment for 10 years, no recurrences were identified using whole body scans. A partial tumor resection was performed and the histological diagnosis was an adenocarcinoma from breast cancer. As no extracranial lesions were found, gamma-knife irradiation was performed, without additional systemic chemotherapy. One month posttreatment, the tumors dramatically reduced in size and the patient completely recovered from cerebellar ataxia. Systemic chemotherapy is not always required for brain metastasis from breast cancer with a long interval period, as long as no evidence of extracranial recurrence is detected.
Keyword
MeSH Terms
Figure
-

Figure 1 Magnetic resonance imaging on admission. (A, B) Gadolinium (gadopentetate dimeglumine)-enhanced T1 weighted images revealed enhanced lesions in both cerebellar hemispheres (A, axial view; B, coronal view). The right side lesion was about 3 cm in longitudinal length and the left side was 8 mm. (C) The T2 weighted image showed the mass with iso- to high-signal with little brain edema around the tumor. (D) In the diffusion-weighted image the right tumor mass possessed an iso-signal but the left has a high signal. The forth ventricle was not compressed by the mass, suggesting the invading character of the tumor.
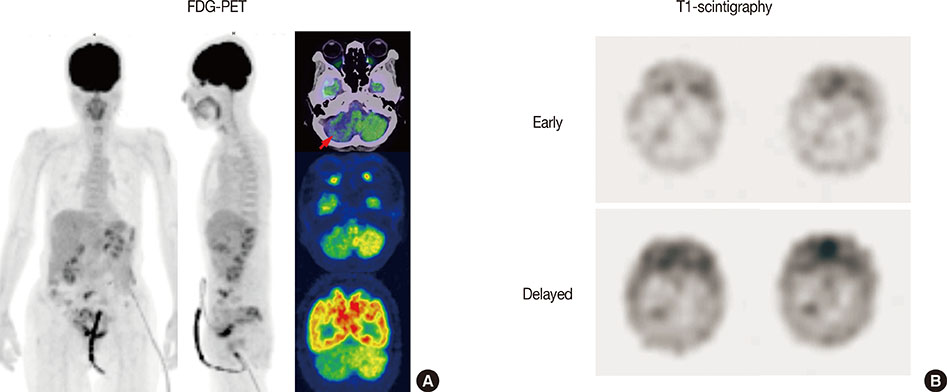
Figure 2 Radionuclide imaging for metastasis. (A) Fluorodeoxyglucose-positron emission tomography (FDG-PET). No evidence of metastasis was identified in a whole body scan. The uptake of FDG was much less in the right cerebellar hemisphere than in the left one. (B) Thallium 201 (201Tl)-scintigraphy. The uptake of Tl was only observed in the right cerebellar lesion in both early and delayed phases, and uptake was clearer in the delayed phase. Retention index (delayed/early) of the lesion was 1.73.

Figure 3 Surgical view. (A) The whitish extra-axial tumor (black arrow) can be seen attaching to the dura mater. (B) The tumor was extremely hard and firm without a clear border with normal brain tissue.
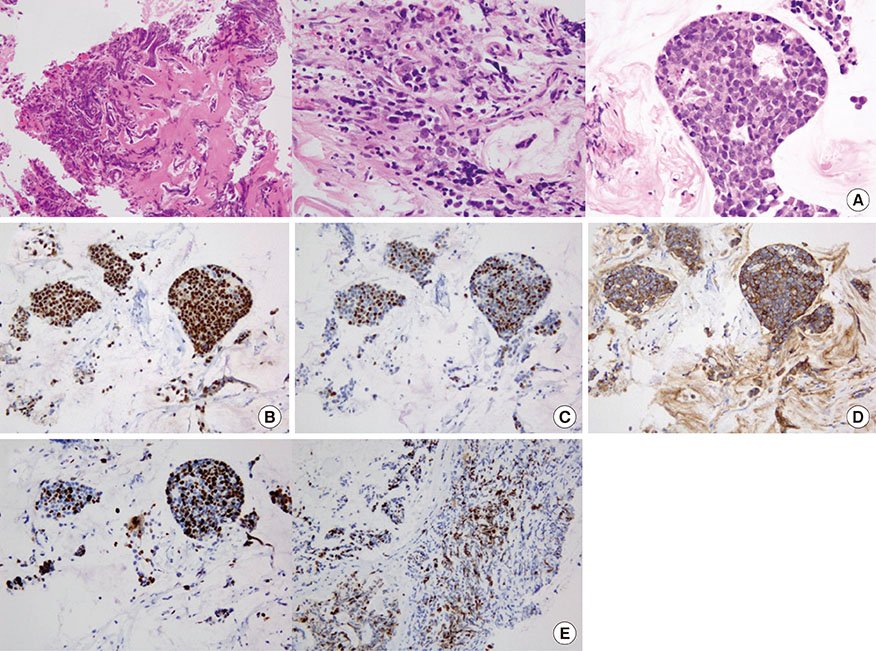
Figure 4 Histology. (A) Cellularity of the tumor is extremely high with a strong atypical appearance and mitosis that is compatible with adenocarcinomas (H&E stain, ×10 in the left, ×40 in the middle and the right). (B) The tumor presented estrogen receptor (IHC, ×20), (C) progesterone receptor (IHC, ×20), and (D) human epidermal growth factor receptor 2 (IHC, ×20) positive (triple-positive). (E) The Ki-67 proliferative index was extremely high, 40% to 60% (IHC, ×20 in the left, ×10 in the right). H&E=hematoxylin and eosin; IHC=immunohistochemistry.
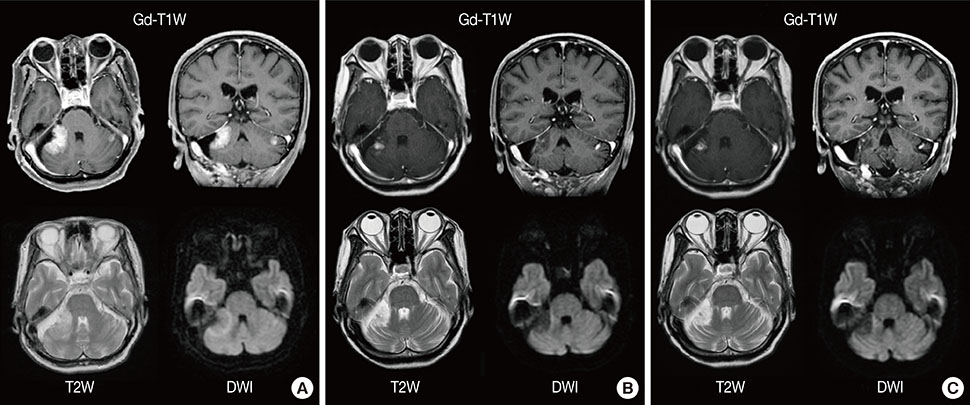
Figure 5 Follow-up magnetic resonance imaging (MRI) before and after surgery and gamma-knife radiation. (A) MRI before gamma-knife radiation. A small piece of tumor was resected and no sign of cerebral spinal fluid seeding was identified. (B) MRI 1 month after gamma-knife radiation. The size of the right cerebellar tumor decreased remarkably following treatment. The right irradiated lesion had a high signal in T2 weighted image (T2W) and a low signal in diffusion-weighted image (DWI), showing the necrotic change of the tumor. (C) MRI 5 months after gamma-knife radiation. The cerebellar metastatic lesions are still identified on MRI (Gd-T1W); however, the size of these lesions and edema around the tumor do not change at all. Gd-T1W=gadolinium (gadopentetate dimeglumine)-enhanced T1 weighted image.
Reference
-
1. De Ieso PB, Schick U, Rosenfelder N, Mohammed K, Ross GM. Breast cancer brain metastases: a 12 year review of treatment outcomes. Breast. 2015; 24:426–433.2. Rostami R, Mittal S, Rostami P, Tavassoli F, Jabbari B. Brain metastasis in breast cancer: a comprehensive literature review. J Neurooncol. 2016; 127:407–414.
Article3. Brogi E, Murphy CG, Johnson ML, Conlin AK, Hsu M, Patil S, et al. Breast carcinoma with brain metastases: clinical analysis and immunoprofile on tissue microarrays. Ann Oncol. 2011; 22:2597–2603.
Article4. Patanaphan V, Salazar OM, Risco R. Breast cancer: metastatic patterns and their prognosis. South Med J. 1988; 81:1109–1112.5. Park HS, Kim S, Kim K, Yoo H, Chae BJ, Bae JS, et al. Pattern of distant recurrence according to the molecular subtypes in Korean women with breast cancer. World J Surg Oncol. 2012; 10:4.
Article6. Pestalozzi BC, Zahrieh D, Price KN, Holmberg SB, Lindtner J, Collins J, et al. Identifying breast cancer patients at risk for central nervous system (CNS) metastases in trials of the International Breast Cancer Study Group (IBCSG). Ann Oncol. 2006; 17:935–944.
Article7. Swain SM, Baselga J, Kim SB, Ro J, Semiglazov V, Campone M, et al. Pertuzumab, trastuzumab, and docetaxel in HER2-positive metastatic breast cancer. N Engl J Med. 2015; 372:724–734.
Article8. Pors H, von Eyben FE, Sørensen OS, Larsen M. Longterm remission of multiple brain metastases with tamoxifen. J Neurooncol. 1991; 10:173–177.
Article9. Crivellari D, Pagani O, Veronesi A, Lombardi D, Nolè F, Thürlimann B, et al. High incidence of central nervous system involvement in patients with metastatic or locally advanced breast cancer treated with epirubicin and docetaxel. Ann Oncol. 2001; 12:353–356.
Article10. Larsen PB, Kümler I, Nielsen DL. A systematic review of trastuzumab and lapatinib in the treatment of women with brain metastases from HER2-positive breast cancer. Cancer Treat Rev. 2013; 39:720–727.
Article11. Nieder C, Oehlke O, Hintz M, Grosu AL. The challenge of durable brain control in patients with brain-only metastases from breast cancer. Springerplus. 2015; 4:585.
Article12. Madhup R, Kirti S, Bhatt ML, Srivastava PK, Srivastava M, Kumar S. Letrozole for brain and scalp metastases from breast cancer: a case report. Breast. 2006; 15:440–442.13. Ogawa K, Yoshii Y, Nishimaki T, Tamaki N, Miyaguni T, Tsuchida Y, et al. Treatment and prognosis of brain metastases from breast cancer. J Neurooncol. 2008; 86:231–238.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Pancreatic Metastasis from Invasive Ductal Carcinoma of the Breast
- The Impact of Local and Regional Recurrence on Distant Metastasis and Survival in Patients Treated with Breast Conservation Therapy
- Colon Obstruction due to Colonic Metastasis of a Breast Carcinoma
- Breast Cancer to Meningioma: A Rare Case of Tumor-to-Tumor Metastasis
- Rapid Progression of Duodenal Metastasis from Invasive Lobular Breast Carcinoma
