Submucosal Esophageal Metastasis in a Patient with Poorly Differentiated Thyroid Carcinoma: a Case Report
- Affiliations
-
- 1Department of General Surgery, Presbyterian Medical Center, Jeonju, Korea. raw93@paran.com
- KMID: 2389593
- DOI: http://doi.org/10.16956/jes.2017.17.3.131
Abstract
- We report an unusual case of esophageal metastasis protruding through the submucosa from a poorly differentiated thyroid carcinoma (PDTC). A PDTC is a very rare thyroid carcinoma subtype. A 68-year-old woman with PDTC exhibited recurrence at the thyroidectomy site and esophageal metastatic mass despite finishing the first treatment and undergoing regular follow-up. She received additional resective treatment with modified radical neck dissection for the recurrent neck nodes and endoscopic submucosal resection for the esophageal protruding mass. To our knowledge, no case of esophageal metastasis protruding through the submucosa from a PDTC has been previously reported.
Keyword
MeSH Terms
Figure
-
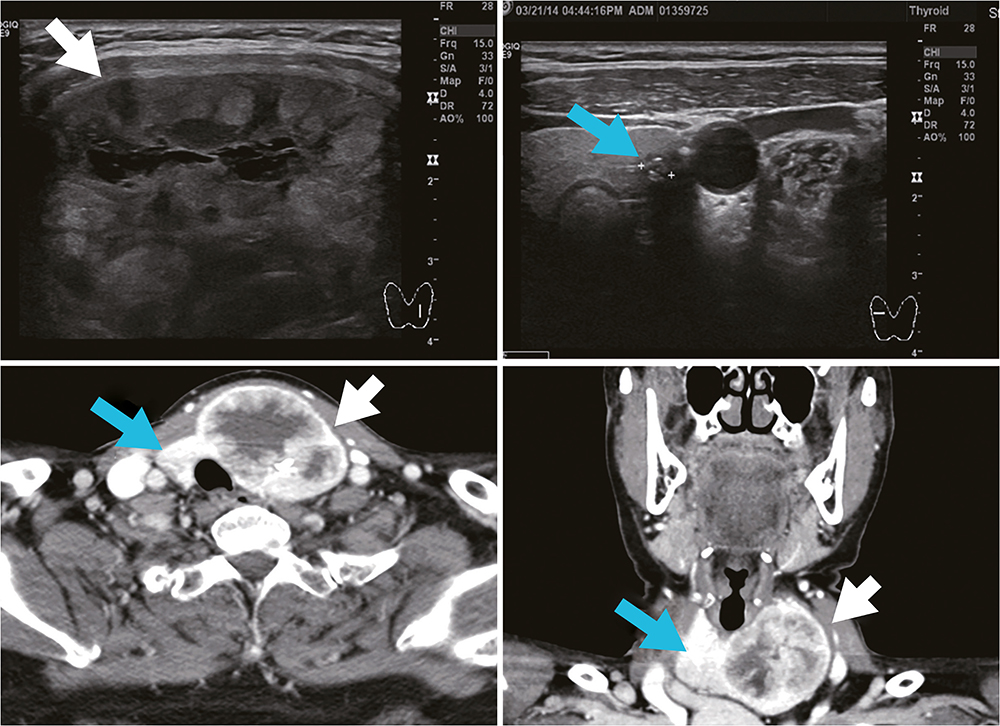
Fig. 1 Pre-operative thyroid ultrasound and CT scan. Right thyroid nodule shows a small central calcification in the upper aspect (blue arrow). Left lobe showed a large 5.2-cm mixed complex type mass of the whole thyroid (white arrow). CT = computed tomography.
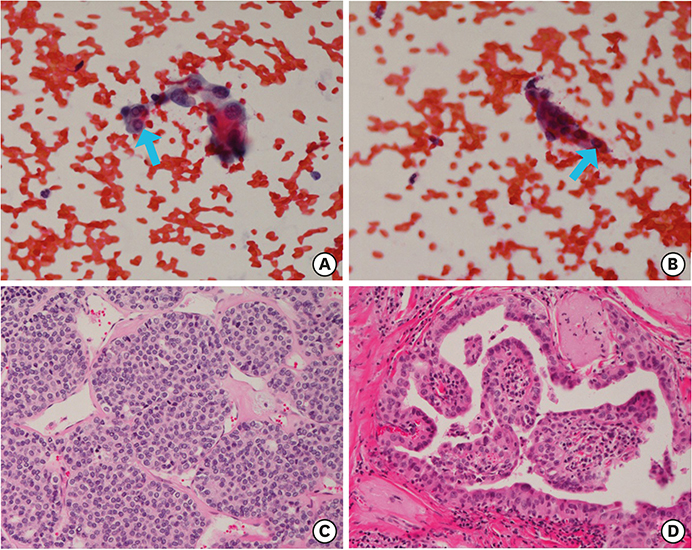
Fig. 2 (A) FNAC slide in left thyroid huge mass: intranuclear inclusions. And very few cellularity (×400). (B) FNAC slid in right thyroid mass: intranuclear inclusion (×400). (C) Insular type PDTC in left thyroid (×200). (D) Papillary thyroid carcinoma in right thyroid (×200). FNAC = fine needle aspiration cytology; PDTC = poorly differentiated thyroid carcinoma.
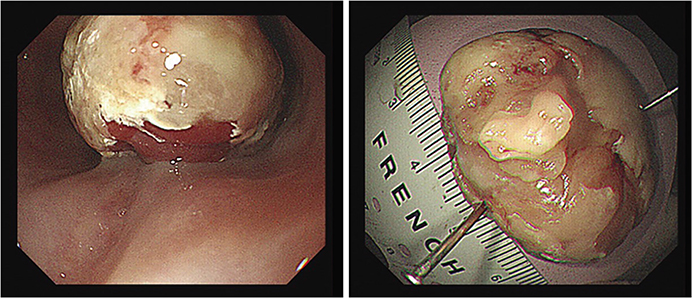
Fig. 3 Endoscopic evaluation of luminal protruding mass in esophagus.
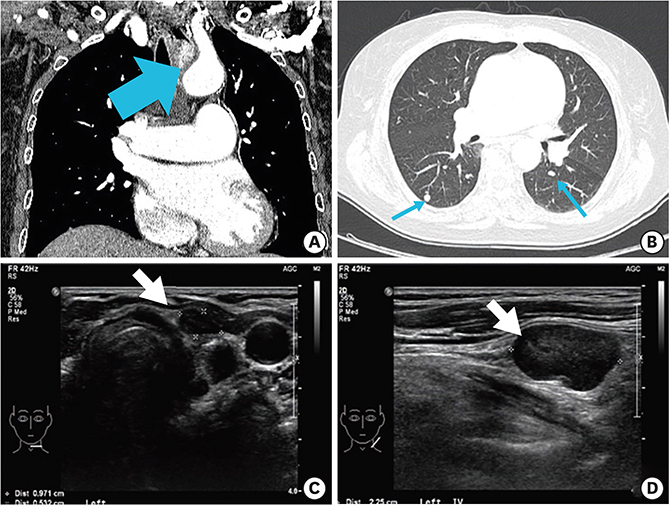
Fig. 4 (A) Esophageal protruding mass (blue arrow). (B) Both lung metastases (blue arrows). (C, D) Post-thyroidectomy site recurrent lymph node enlargement at 18 months (white arrows).

Fig. 5 PET-CT scan. Uptake of post-thyroidectomy site recurrent lymph node (white arrow) and esophageal metastasis (blue arrows). PET = positron emission tomography; CT = computed tomography.
Reference
-
1. Sakamoto A, Kasai N, Sugano H. Poorly differentiated carcinoma of the thyroid. A clinicopathologic entity for a high-risk group of papillary and follicular carcinomas. Cancer. 1983; 52:1849–1855.
Article2. Bongiovanni M, Sadow PM, Faquin WC. Poorly differentiated thyroid carcinoma: a cytologic-histologic review. Adv Anat Pathol. 2009; 16:283–289.3. Volante M, Landolfi S, Chiusa L, Palestini N, Motta M, Codegone A, et al. Poorly differentiated carcinomas of the thyroid with trabecular, insular, and solid patterns: a clinicopathologic study of 183 patients. Cancer. 2004; 100:950–957.
Article4. Wreesmann VB, Ghossein RA, Patel SG, Harris CP, Schnaser EA, Shaha AR, et al. Genome-wide appraisal of thyroid cancer progression. Am J Pathol. 2002; 161:1549–1556.
Article5. Luna-Ortiz K, Hurtado-López LM, Domínguez-Malagón H, Ramírez-Marín R, Zaldivar-Ramírez FR, Herrera-Gomez A, et al. Clinical course of insular thyroid carcinoma. Med Sci Monit. 2004; 10:CR108–CR111.6. Pulcrano M, Boukheris H, Talbot M, Caillou B, Dupuy C, Virion A, et al. Poorly differentiated follicular thyroid carcinoma: prognostic factors and relevance of histological classification. Thyroid. 2007; 17:639–646.
Article7. Patel KN, Shaha AR. Poorly differentiated thyroid cancer. Curr Opin Otolaryngol Head Neck Surg. 2014; 22:121–126.
Article8. Onenerk M, Canberk S, Gunes P, Erkan M, Kilicoglu GZ. Oncocytic variant of poorly differentiated thyroid carcinoma: “Is diagnosis possible by fine-needle aspiration?”. Cytojournal. 2016; 13:23.
Article9. Rocha AS, Soares P, Fonseca E, Cameselle-Teijeiro J, Oliveira MC, Sobrinho-Simões M. E-cadherin loss rather than β‐catenin alterations is a common feature of poorly differentiated thyroid carcinomas. Histopathology. 2003; 42:580–587.
Article10. Kane SV, Sharma TP. Cytologic diagnostic approach to poorly differentiated thyroid carcinoma: a single-institution study. Cancer Cytopathol. 2015; 123:82–91.
Article11. Ibrahimpasic T, Ghossein R, Carlson DL, Nixon I, Palmer FL, Shaha AR, et al. Outcomes in patients with poorly differentiated thyroid carcinoma. J Clin Endocrinol Metab. 2014; 99:1245–1252.
Article12. Sobrinho-Simões M, Sambade C, Fonseca E, Soares P. Poorly differentiated carcinomas of the thyroid gland: a review of the clinicopathologic features of a series of 28 cases of a heterogeneous, clinically aggressive group of thyroid tumors. Int J Surg Pathol. 2002; 10:123–131.13. Seoung HG, Kim JH, Choi JC, Kim SM, Kim SS, Kim BH, et al. A case of papillary thyroid cancer recurring as an esophageal submucosal tumor. Chonnam Med J. 2012; 48:60–64.
Article14. Lee MY, Kim SE, Kim HC, Han SH, Shin DH, Kim DH, et al. Direct invasion of thyroid papillary carcinoma to esophagus presenting as an intraluminal polypoid mass which causes hematemesis. Korean J Gastrointest Endosc. 2001; 23:466–469.15. Muñoz de Nova JL, Dworzynska A, Lorente-Poch L, Sancho JJ, Sitges-Serra A. Esophageal recurrence of medullary thyroid carcinoma. Gland Surg. 2015; 4:564–566.16. Lee B, Cook G, John L, Harrington K, Nutting C. Follicular thyroid carcinoma metastasis to the esophagus detected by 18FDG PET/CT. Thyroid. 2008; 18:267–271.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Metastasis of Poorly Differentiated Thyroid Carcinoma to the Sternum: A Case Report
- A Case of Papillary Thyroid Cancer Recurring as an Esophageal Submucosal Tumor
- A Case of Scalp Metastasis from Follicular Thyroid Carcinoma
- Fine Needle Aspiration Cytoloy of Poorly Differentiated "Insular" Carcinoma of the Thyroid: A Case Report
- Successful Treatment of Cavernous Sinus Metastasis from Follicular Thyroid Carcinoma with Lenvatinib
