A Case of Grisel Syndrome Showing No Underlying Laxity of the Atlanto-axial Joint
- Affiliations
-
- 1The Center for Torticollis, Department of Physical Medicine and Rehabilitation, Ajou University School of Medicine, Suwon, Korea. syyim@ajou.ac.kr
- KMID: 2389470
- DOI: http://doi.org/10.5535/arm.2017.41.3.511
Abstract
- Grisel syndrome is a rare, non-traumatic atlanto-axial subluxation associated with an inflammatory or infectious process in the upper neck. According to the two-hit hypothesis, which is widely accepted for the pathogenesis of Grisel syndrome, preexisting ligamentous laxity of the atlanto-axial joint is regarded as the first hit. An inflammatory or infectious process of the atlanto-axial joint acts as the second hit, resulting in non-traumatic atlanto-axial subluxation. We report on a 6-year-old girl with atlanto-axial subluxation following retropharyngeal and cervical lymphadenitis. She was diagnosed with Grisel syndrome, for which an initial computed tomography did not show any preexisting ligamentous laxity of the atlanto-axial joint. A literature review found only 4 case reports on Grisel syndrome with an initially normal atlanto-axial joint. The present case offers some evidence that a single hit, such as inflammatory changes in the atlanto-axial joint, might cause Grisel syndrome, even without underlying ligamentous laxity.
Keyword
MeSH Terms
Figure
-
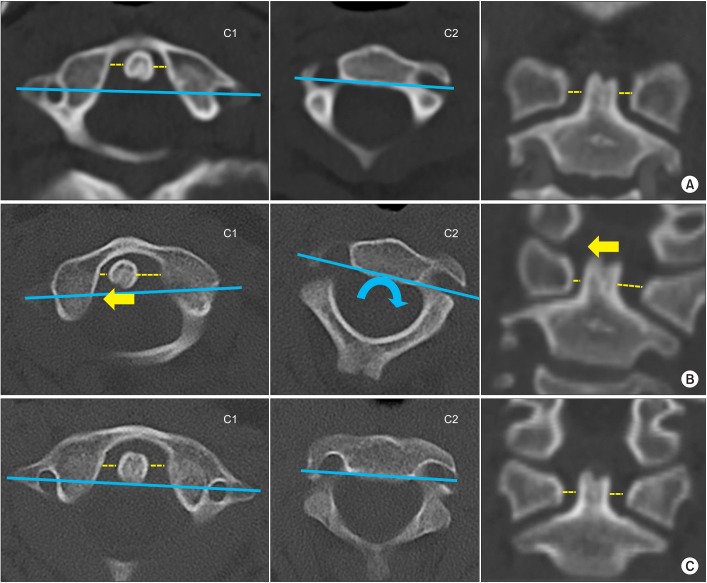
Fig. 1 Serial neck computed tomography (CT). (A) The initial CT on admission shows a normal alignment of the atlanto-axial joint with symmetric lateral atlanto-dens interval and without rotation of the atlanto-axial joint. (B) CT taken after the onset of torticollis shows rotation of the atlanto-axial joint (blue curved arrow) with a lateral shift of the dens toward the right (yellow arrow). (C) CT on the 28th hospital day shows a normal alignment of the atlanto-axial joint. C1, the atlas; C2, the axis; blue line, a line connecting bilateral transverse foramina of the atlas and the axis; yellow dotted line, the lateral atlanto-dens interval.

Fig. 2 A 6-year-old girl with Grisel syndrome showing abnormal head posture.

Fig. 3 Radiographic studies showing inflammatory changes of the soft tissue. (A) Computed tomography with contrast shows a diffuse, low attenuating lesion in the retropharyngeal space, indicating a fluid collection due to inflammation (white arrow). (B) Axial gadolinium-enhanced T1-weighted magnetic resonance imaging (MRI) shows a fluid collection in the retropharyngeal space (white arrow). (C) Sagittal gadolinium-enhanced T1-weighted MRI shows abnormal enhancement of ligaments of the atlanto-axial joint (black arrow) and posterior longitudinal ligament at the level of the C2 vertebra (black arrow head), suggesting inflammatory changes of the soft tissue. (D) Sagittal T2-weighted MRI shows a fluid collection in the atlanto-axial joint space (white arrow head).
Reference
-
1. Karkos PD, Benton J, Leong SC, Mushi E, Sivaji N, Assimakopoulos DA. Grisel's syndrome in otolaryngology: a systematic review. Int J Pediatr Otorhinolaryngol. 2007; 71:1823–1827. PMID: 17706297.
Article2. Deichmueller CM, Welkoborsky HJ. Grisel's syndrome: a rare complication following “small” operations and infections in the ENT region. Eur Arch Otorhinolaryngol. 2010; 267:1467–1473. PMID: 20390289.3. Park SH, Park SH, Lee SH. Grisel syndrome: pathophysiological evidence from magnetic resonance imaging findings. Ann Rehabil Med. 2013; 37:713–716. PMID: 24236260.
Article4. Wilson MJ, Michele AA, Jacobson EW. Spontaneous dislocation of the atlanto-axial articulation, including a report of a case with quadriplegia. J Bone Joint Surg Am. 1940; 22:698–707.5. Battiata AP, Pazos G. Grisel's syndrome: the two-hit hypothesis: a case report and literature review. Ear Nose Throat J. 2004; 83:553–555. PMID: 15487635.6. Osiro S, Tiwari KJ, Matusz P, Gielecki J, Tubbs RS, Loukas M. Grisel's syndrome: a comprehensive review with focus on pathogenesis, natural history, and current treatment options. Childs Nerv Syst. 2012; 28:821–825. PMID: 22293953.
Article7. Parke WW, Rothman RH, Brown MD. The pharyngovertebral veins: an anatomical rationale for Grisel's syndrome. J Bone Joint Surg Am. 1984; 66:568–574. PMID: 6707036.8. Jackson H. The diagnosis of minimal atlanto-axial subluxation. Br J Radiol. 1950; 23:672–674. PMID: 14783688.
Article9. Kerolus M, Jeans EB, Fontes RB, Deutsch H, Traynelis VC. Atlantoaxial instability of inflammatory origin in adults: case reports, literature review, and rationale for early surgical intervention. Neurosurgery. 2015; 76:E226–E232. PMID: 25255263.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Atlanto-Axial Joint Subluxation Following Tonsillectomy in Patient of Tonsillar Cancer with Preoperative Radiotherapy: Grisel's Syndrome
- A Case of Grisel’s Syndrome After Tonsillectomy and Adenoidectomy
- Quadriplegia and Dyspnea Caused by Os Odontoideum in a Down Syndrome Patient: A case report
- A Case of Grisel’s Syndrome Following Tonsillectomy and Adenoidectomy
- Non-traumatic Atlanto-axial Rotatory Subluxation: A Case Report
