A Case of Polymyositis Associated with Immunoglobulin A Nephropathy
- Affiliations
-
- 1Division of Rheumatology, Department of Internal Medicine, Yonsei University College of Medicine, Seoul, Korea.
- 2Department of Pathology, Yonsei University College of Medicine, Seoul, Korea.
- 3Division of Nephrology, Department of Internal Medicine, National Health Insurance Service Ilsan Hospital, Goyang, Korea.
- 4Department of Pathology, National Health Insurance Service Ilsan Hospital, Goyang, Korea.
- 5Division of Rheumatology, Department of Internal Medicine, National Health Insurance Service Ilsan Hospital, Goyang, Korea. jinsulog@naver.com
- KMID: 2389066
- DOI: http://doi.org/10.4078/jrd.2017.24.4.241
Abstract
- Polymyositis (PM) is a chronic inflammatory disease that predominantly affects muscles. Systemic organ involvement, including the respiratory and gastrointestinal tracts, is frequently observed in PM, but renal involvement is rare. Herein, we report the case of a 56-year-old woman presenting with weight gain, edema, and generalized myalgia. Laboratory tests revealed elevated creatinine kinase level, hypoalbuminemia, and proteinuria. Histopathological examination of muscle biopsy revealed inflammatory myositis, and a renal biopsy confirmed immunoglobulin A (IgA) nephropathy. Based on the clinico-pathological results, the patient was diagnosed with PM with IgA nephropathy. This is a report of a rare occurrence of IgA nephropathy in a patient with PM presenting with chronic glomerulonephritis.
Keyword
MeSH Terms
Figure
-

Figure 1. Muscle biopsy. (A) Light microgram of a muscle biopsy specimen (H&E, ×40). (B) Light microgram showing inflammatory cell infiltrates (black arrows) scattered throughout the endomysium, invading individual muscle fibers (H&E, ×200).(C) On immunohistochemistry, the inflammatory cells express leukocyte common antigen (black arrows) (Immunohistochemistry,×200). (D) Anti CD 68 staining of the muscle biopsy specimen (Immunohistochemistry, ×200).
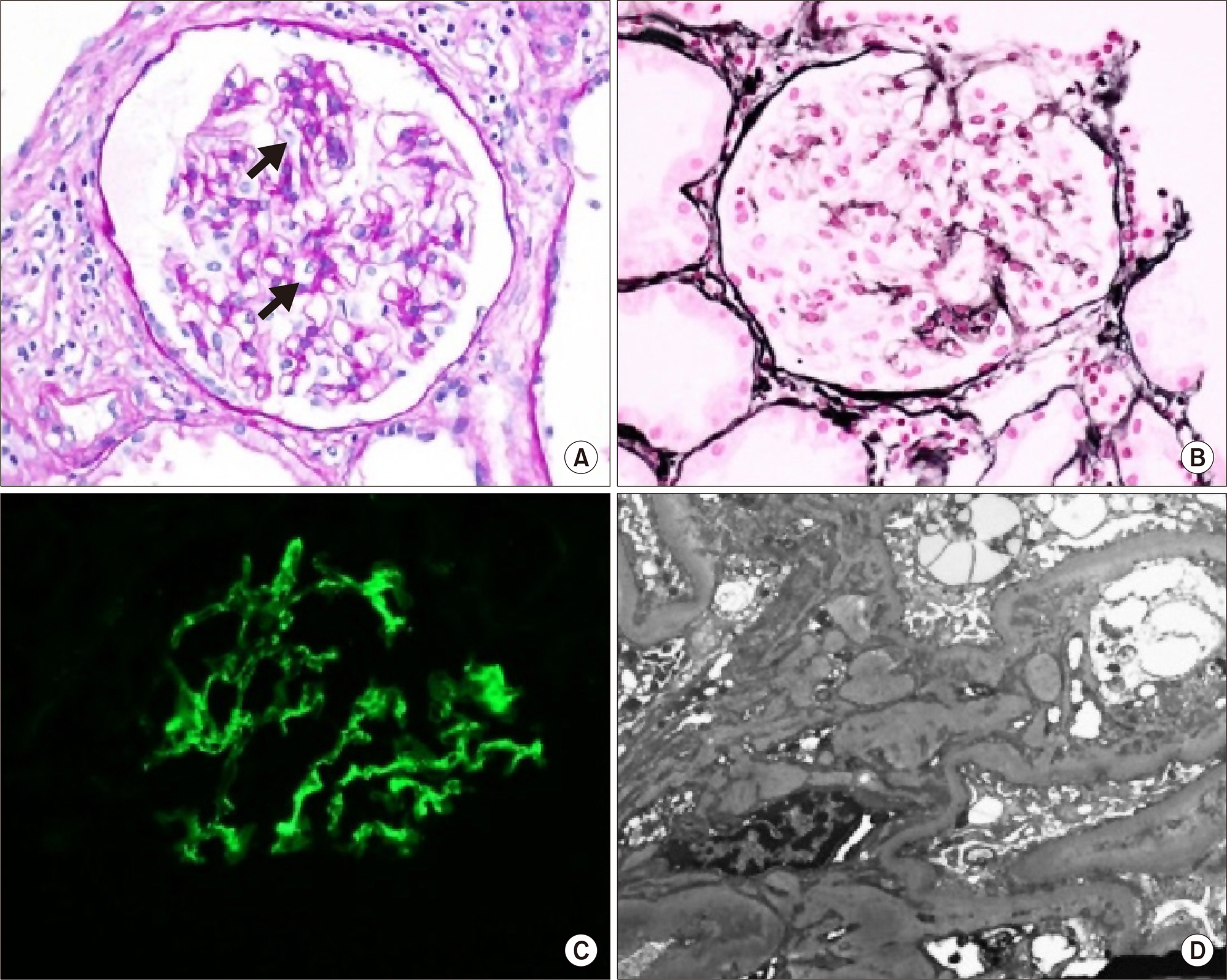
Figure 2. Renal biopsy. (A) Light microgram showing mild mesangial expansion (black arrows) without cellular proliferation (Periodic acid Schiff, ×400). (B) Some glomeruli showed segmental sclerotic change and synechia with Bowman's capsule (PAS-silver stain, ×400). (C) Immunofluorescence staining revealed moderate positivity for IgA on the mesangium and para-mesangium (Immunofluorescence staining, ×400). (D) Electron microgram demonstrating deposits in the mesangium and para-mesangium (Uranyl acetate, ×6,000).
Reference
-
1. Bohan A, Peter JB. Polymyositis and dermatomyositis (first of two parts). N Engl J Med. 1975; 292:344–7.2. Takizawa Y, Kanda H, Sato K, Kawahata K, Yamaguchi A, Uozaki H, et al. Polymyositis associated with focal mesangial proliferative glomerulonephritis with depositions of immune complexes. Clin Rheumatol. 2007; 26:792–6.
Article3. Cucchiari D, Angelini C. Renal involvement in idiopathic inflammatory myopathies. Clin Rev Allergy Immunol. 2017; 52:99–107.
Article4. Wu Y, Chhaya S, Hurowitz B, Ardiles T, Carlson R. Clinically amyopathic dermatomyositis complicated by pleural effusion case report, literature review, and proposed mechanism. Bull Hosp Jt Dis (2013). 2015; 73:217–20.5. Qian Y, Ren H, Zhang W, Chen N. Clinical features of polymyositis and dermatomyositis in four patients with renal involvement as mainly presentation. Zhonghua Nei Ke Za Zhi. 2009; 48:930–2.6. Nickavar A, Mehr Azma M. Nephrotic syndrome and juvenile dermatomyositis. Rheumatol Int. 2012; 32:2933–5.
Article7. Findlay AR, Goyal NA, Mozaffar T. An overview of polymyositis and dermatomyositis. Muscle Nerve. 2015; 51:638–56.
Article8. Couvrat-Desvergnes G, Masseau A, Benveniste O, Bruel A, Hervier B, Mussini JM, et al. The spectrum of renal involvement in patients with inflammatory myopathies. Medicine (Baltimore). 2014; 93:33–41.
Article9. Shin DH, Lim BJ, Han IM, Han SG, Kwon YE, Park KS, et al. Glomerular IgG deposition predicts renal outcome in patients with IgA nephropathy. Mod Pathol. 2016; 29:743–52.
Article10. Civilibal M, Selcuk Duru N, Ozagari A, Durali K, Elevli M. Immunoglobulin A nephropathy associated with juvenile dermatomyositis. Pediatr Nephrol. 2009; 24:2073–5.
Article11. Pouria S, Barratt J. Secondary IgA nephropathy. Semin Nephrol. 2008; 28:27–37.
Article12. Stertz G. Polymyositis. Berl Klin Wochenschr. 1916; 53:489.13. Levine SM. Cancer and myositis: new insights into an old association. Curr Opin Rheumatol. 2006; 18:620–4.
Article14. Barros TB, de Souza FH, Malheiros DM, Levy-Neto M, Shinjo SK. IgA nephropathy and polymyositis: a rare association. Rev Bras Reumatol. 2014; 54:231–3.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Eosinophilic Polymyositis in a Patient with IgA Nephropathy
- A Case of Overlap Syndrome of Dermatomyositis and Sjogren's Syndrome associated with IgA Nephropathy
- A Case of Polymyositis Associated with Primary Biliary Cirrhosis
- A Case of Polymyositis Treated with Intravenous Immunoglobulin
- A Case of Familial IgA Nephropathy
