Cancer Res Treat.
2017 Jul;49(3):669-677. 10.4143/crt.2016.354.
Dose-Response Relationship between Radiation Dose and Loco-regional Control in Patients with Stage II-III Esophageal Cancer Treated with Definitive Chemoradiotherapy
- Affiliations
-
- 1Department of Radiation Oncology, Yonsei University College of Medicine, Seoul, Korea. cglee1023@yuhs.ac
- 2Department of Radiation Oncology, National Cancer Center, Goyang, Korea.
- 3Division of Gastroenterology, Department of Internal Medicine, Yonsei University College of Medicine, Seoul, Korea.
- 4Division of Medical Oncology, Department of Internal Medicine, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 2388312
- DOI: http://doi.org/10.4143/crt.2016.354
Abstract
- PURPOSE
The correlation between radiation dose and loco-regional control (LRC) was evaluated in patients with stage II-III esophageal cancer treated with definitive concurrent chemoradiotherapy (CRT).
MATERIALS AND METHODS
Medical records of 236 stage II-III esophageal cancer patients treated with definitive CRT at Yonsei Cancer Center between 1994 and 2013 were retrospectively reviewed. Among these, 120 received a radiation dose of < 60 Gy (standard-dose group), while 116 received ≥ 60 Gy (high-dose group). The median doses of radiation in the standard- and high-dose groups were 50.4 and 63 Gy, respectively. Concurrent 5-fluorouracil/cisplatin chemotherapy was administered to most patients.
RESULTS
There were no differences in patient characteristics between the two groups except for high Karnofsky performance status and lower-thoracic lesions being more prevalent in the standard-dose group. The median progression-free survival (PFS) and overall survival (OS) times were 13.2 months and 26.2 months, respectively. Patients in the high-dose group had significantly better 2-year LRC (69.1% vs. 50.3%, p=0.002), median PFS (16.7 months vs. 11.7 months, p=0.029), and median OS (35.1 months vs. 22.3 months, p=0.043). Additionally, LRC exhibited a dose-response relationship and the complete response rate was significantly higher in the high-dose group (p=0.006). There were no significant differences in treatment-related toxicities between the groups.
CONCLUSION
A higher radiation dose (> 60 Gy) is associated with increased LRC, PFS, and OS in patients with stage II-III esophageal cancer treated with definitive CRT.
MeSH Terms
Figure
-
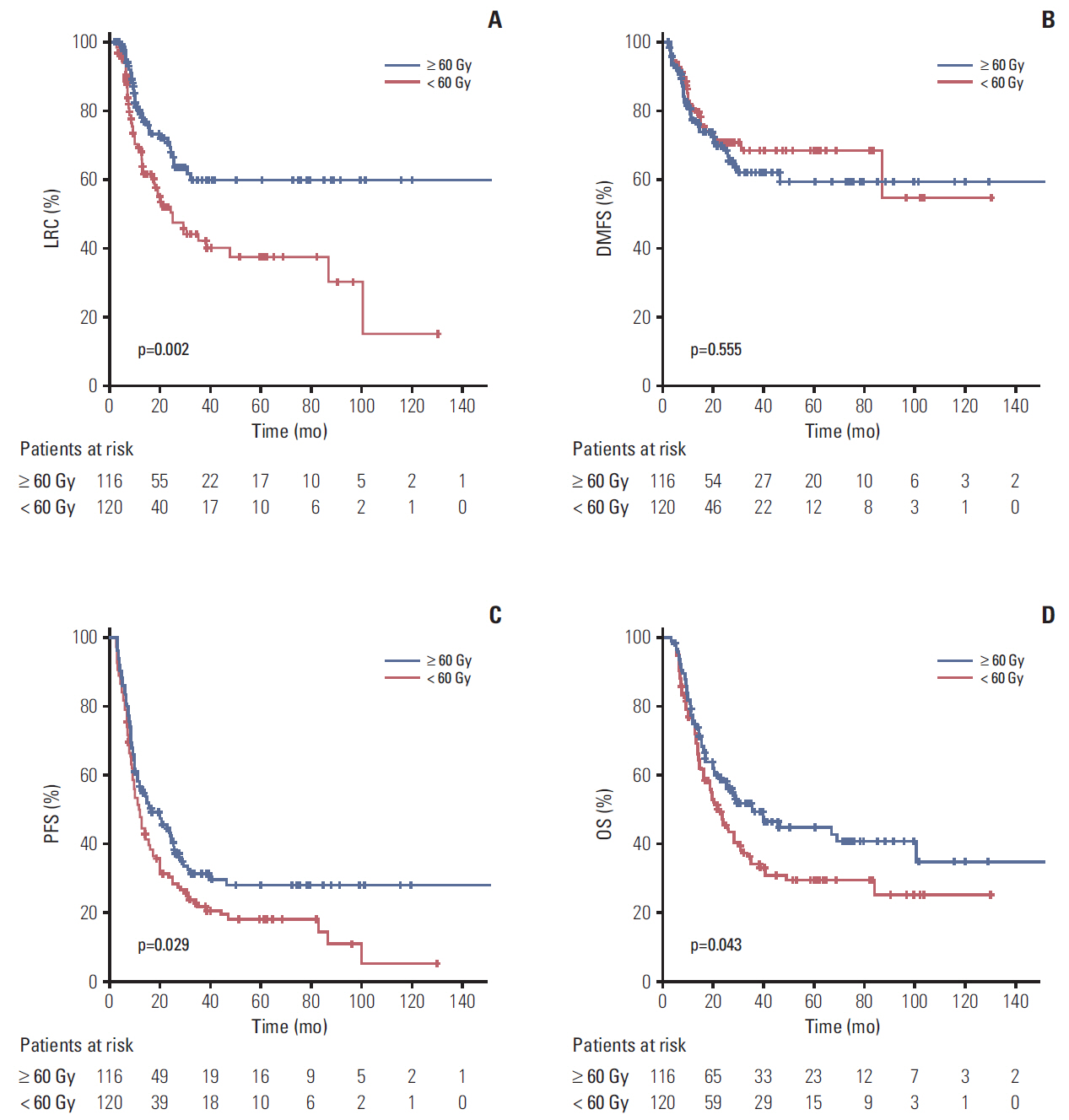
Fig. 1. Kaplan-Meier curves of locoregional control (LRC) (A), distant metastasis-free survival (DMFS) (B), progression-free survival (PFS) (C), and overall survival (OS) (D).
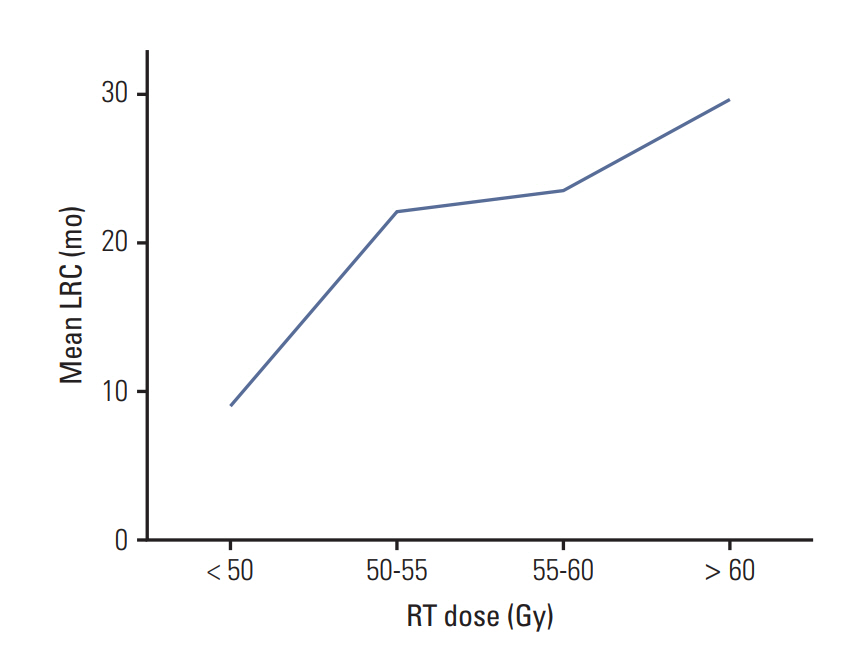
Fig. 2. Dose response relationship between radiotherapy (RT) dose and loco-regional control (LRC) durations.
Cited by 1 articles
-
Intensity-Modulated Radiotherapy versus Three-Dimensional Conformal Radiotherapy in Definitive Chemoradiotherapy for Cervical Esophageal Squamous Cell Carcinoma: Comparison of Survival Outcomes and Toxicities
Nai-Bin Chen, Bo Qiu, Jun Zhang, Meng-Yun Qiang, Yu-Jia Zhu, Bin Wang, Jin-Yu Guo, Ling-Zhi Cai, Shao-Min Huang, Meng-Zhong Liu, Qun Li, Yong-Hong Hu, Qi-Wen Li, Hui Liu
Cancer Res Treat. 2020;52(1):31-40. doi: 10.4143/crt.2018.624.
Reference
-
References
1. Global Burden of Disease Cancer Collaboration, Fitzmaurice C, Dicker D, Pain A, Hamavid H, Moradi-Lakeh M, et al. The global burden of cancer 2013. JAMA Oncol. 2015; 1:505–27.2. Enzinger PC, Mayer RJ. Esophageal cancer. N Engl J Med. 2003; 349:2241–52.
Article3. Bosset JF, Gignoux M, Triboulet JP, Tiret E, Mantion G, Elias D, et al. Chemoradiotherapy followed by surgery compared with surgery alone in squamous-cell cancer of the esophagus. N Engl J Med. 1997; 337:161–7.
Article4. Tepper J, Krasna MJ, Niedzwiecki D, Hollis D, Reed CE, Goldberg R, et al. Phase III trial of trimodality therapy with cisplatin, fluorouracil, radiotherapy, and surgery compared with surgery alone for esophageal cancer: CALGB 9781. J Clin Oncol. 2008; 26:1086–92.
Article5. Cooper JS, Guo MD, Herskovic A, Macdonald JS, Martenson JA Jr, Al-Sarraf M, et al. Chemoradiotherapy of locally advanced esophageal cancer: long-term follow-up of a prospective randomized trial (RTOG 85-01). Radiation Therapy Oncology Group. JAMA. 1999; 281:1623–7.
Article6. al-Sarraf M, Martz K, Herskovic A, Leichman L, Brindle JS, Vaitkevicius VK, et al. Progress report of combined chemoradiotherapy versus radiotherapy alone in patients with esophageal cancer: an intergroup study. J Clin Oncol. 1997; 15:277–84.
Article7. Herskovic A, Martz K, al-Sarraf M, Leichman L, Brindle J, Vaitkevicius V, et al. Combined chemotherapy and radiotherapy compared with radiotherapy alone in patients with cancer of the esophagus. N Engl J Med. 1992; 326:1593–8.
Article8. Minsky BD, Pajak TF, Ginsberg RJ, Pisansky TM, Martenson J, Komaki R, et al. INT 0123 (Radiation Therapy Oncology Group 94-05) phase III trial of combined-modality therapy for esophageal cancer: high-dose versus standard-dose radiation therapy. J Clin Oncol. 2002; 20:1167–74.
Article9. Kachnic LA, Winter K, Wasserman T, Kelsen D, Ginsberg R, Pisansky TM, et al. Longitudinal quality-of-life analysis of RTOG 94-05 (Int 0123): a phase III trial of definitive chemoradiotherapy for esophageal cancer. Gastrointest Cancer Res. 2011; 4:45–52.10. National Comprehensive Cancer Network. NCCN guideline [Internet]. Fort Washington, PA: National Comprehensive Cancer Network;2016. [cited 2016 Jan 4]. Available from: http://www.nccn.org/professionals/physician_gls/pdf/esophageal.pdf.11. Fletcher GH. Keynote address: the scientific basis of the present and future practice of clinical radiotherapy. Int J Radiat Oncol Biol Phys. 1983; 9:1073–82.
Article12. Halperin EC, Wazer DE, Perez CA, Brady LW. Perez and Brady's principles and practice of radiation oncology. 6th ed. Philadelphia, PA: Lippincott Williams & Wilkins;2013.13. Seung SK, Smith JW, Molendyk J, Bader SB, Phillips M, Regan J, et al. Selective dose escalation of chemoradiotherapy for esophageal cancer: role of treatment intensification. Semin Oncol. 2004; 31(6 Suppl 18):13–9.
Article14. Zhang Z, Liao Z, Jin J, Ajani J, Chang JY, Jeter M, et al. Dose-response relationship in locoregional control for patients with stage II-III esophageal cancer treated with concurrent chemotherapy and radiotherapy. Int J Radiat Oncol Biol Phys. 2005; 61:656–64.
Article15. Song T, Liang X, Fang M, Wu S. High-dose versus conventional-dose irradiation in cisplatin-based definitive concurrent chemoradiotherapy for esophageal cancer: a systematic review and pooled analysis. Expert Rev Anticancer Ther. 2015; 15:1157–69.
Article16. Suh YG, Lee IJ, Koom WS, Cha J, Lee JY, Kim SK, et al. High-dose versus standard-dose radiotherapy with concurrent chemotherapy in stages II-III esophageal cancer. Jpn J Clin Oncol. 2014; 44:534–40.
Article17. Sasamoto R, Sakai K, Inakoshi H, Sueyama H, Saito M, Sugita T, et al. Long-term results of chemoradiotherapy for locally advanced esophageal cancer, using daily low-dose 5-fluorouracil and cis-diammine-dichloro-platinum (CDDP). Int J Clin Oncol. 2007; 12:25–30.
Article18. Bedenne L, Michel P, Bouche O, Milan C, Mariette C, Conroy T, et al. Chemoradiation followed by surgery compared with chemoradiation alone in squamous cancer of the esophagus: FFCD 9102. J Clin Oncol. 2007; 25:1160–8.
Article19. Vincent J, Mariette C, Pezet D, Huet E, Bonnetain F, Bouche O, et al. Early surgery for failure after chemoradiation in operable thoracic oesophageal cancer: analysis of the non-randomised patients in FFCD 9102 phase III trial: Chemoradiation followed by surgery versus chemoradiation alone. Eur J Cancer. 2015; 51:1683–93.
Article20. Hurmuzlu M, Monge OR, Smaaland R, Viste A. High-dose definitive concomitant chemoradiotherapy in non-metastatic locally advanced esophageal cancer: toxicity and outcome. Dis Esophagus. 2010; 23:244–52.
Article21. Darby SC, McGale P, Taylor CW, Peto R. Long-term mortality from heart disease and lung cancer after radiotherapy for early breast cancer: prospective cohort study of about 300,000 women in US SEER cancer registries. Lancet Oncol. 2005; 6:557–65.
Article22. Bradley JD, Paulus R, Komaki R, Masters G, Blumenschein G, Schild S, et al. Standard-dose versus high-dose conformal radiotherapy with concurrent and consolidation carboplatin plus paclitaxel with or without cetuximab for patients with stage IIIA or IIIB non-small-cell lung cancer (RTOG 0617): a randomised, two-by-two factorial phase 3 study. Lancet Oncol. 2015; 16:187–99.
Article23. Tucker SL, Liu A, Gomez D, Tang LL, Allen P, Yang J, et al. Impact of heart and lung dose on early survival in patients with non-small cell lung cancer treated with chemoradiation. Radiother Oncol. 2016; 119:495–500.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Prognostic factors of dose-response relationship for nodal control in metastatic lymph nodes of cervical cancer patients undergoing definitive radiotherapy with concurrent chemotherapy
- Impact on Loco-regional Control of Radiochemotherapeutic Sequence and Time to Initiation of Adjuvant Treatment in Stage II/III Rectal Cancer Patients Treated with Postoperative Concurrent Radiochemotherapy
- Salvage Radiotherapy for Loco-regional Recurrence of Esophageal Cancer Following Surgery
- Results of Radiation Therapy for Squamous Cell Carcinoma of the Esophagus
- Definitive Radiotherapy of Non-Small Cell Lung Cancer
