Prevalence and risk indicators of peri-implantitis in Korean patients with a history of periodontal disease: a cross-sectional study
- Affiliations
-
- 1Department of Periodontology, Institute of Oral Bioscience, Chonbuk National University School of Dentistry, Jeonju, Korea. chang@chonbuk.ac.kr
- 2Research Institute of Clinical Medicine of Chonbuk National University-Biomedical Research Institute of Chonbuk National University Hospital, Jeonju, Korea.
- KMID: 2388111
- DOI: http://doi.org/10.5051/jpis.2017.47.4.240
Abstract
- PURPOSE
The aim of this study was to analyze the prevalence and risk indicators of peri-implantitis in Korean patients with history of periodontal disease.
METHODS
A total of 444 patients with 1,485 implants were selected from patients who had been treated at the Department of Periodontology, Chonbuk National University Dental Hospital between July 2014 and June 2015. A group with a history of peri-implantitis (HP) (370 patients with 1,189 implants) and a group with a current peri-implantitis (CP) (318 patients with 1,004 implants) were created based on the radiographic and clinical assessments of implants. The prevalence of peri-implantitis was calculated at both the patient and implant levels. The influence of risk variables on the occurrence of peri-implantitis was analyzed using generalized estimating equations analysis.
RESULTS
The prevalence of peri-implantitis in the HP and CP groups ranged from 6.7% to 19.7%. The cumulative peri-implantitis rate in the HP group estimated with the Kaplan-Meier method was higher than that in the CP group over the follow-up period. Among the patient-related risk variables, supportive periodontal therapy (SPT) was the only significant risk indicator for the occurrence of peri-implantitis in both groups. In the analysis of implant-related variables, implants supporting fixed dental prosthesis (FDP) and implants with subjective discomfort were associated with a higher prevalence of peri-implantitis than single implants and implants without subjective discomfort in the HP group. The presence of subjective discomfort was the only significant implant-related variable predictive of peri-implantitis in the CP group.
CONCLUSIONS
Within the limitations of this study, the prevalence of peri-implantitis in Korean patients with a history of periodontal disease was similar to that reported in other population samples. Regular SPT was important for preventing peri-implantitis. Single implants were found to be less susceptible to peri-implantitis than those supporting FDP. Patients' subjective discomfort was found to be a strong risk indicator for peri-implantitis.
Keyword
MeSH Terms
Figure
-
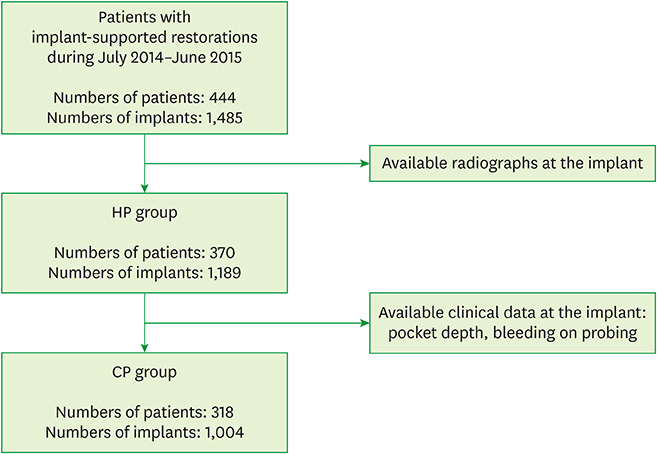
Figure 1 Selection process of the patient groups. HP: history of peri-implantitis, CP: current peri-implantitis.
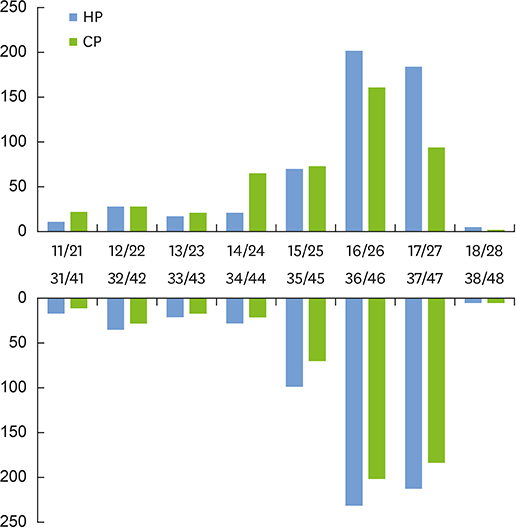
Figure 2 Numbers of implants in the groups with a HP and CP according to implant positions following the Fédération Dentaire Internationale tooth numbering system. HP: history of peri-implantitis, CP: current peri-implantitis.
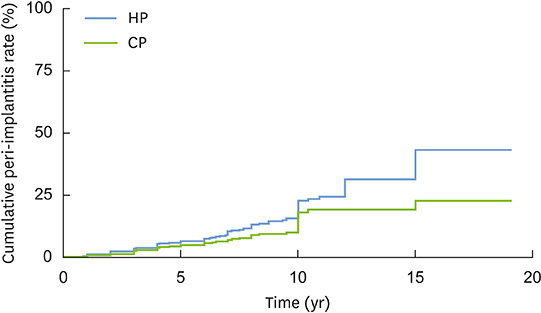
Figure 3 Cumulative peri-implantitis rate at the implant level in groups with a HP and CP over a 19-year follow-up period estimated with the Kaplan-Meier method. HP: history of peri-implantitis, CP: current peri-implantitis.
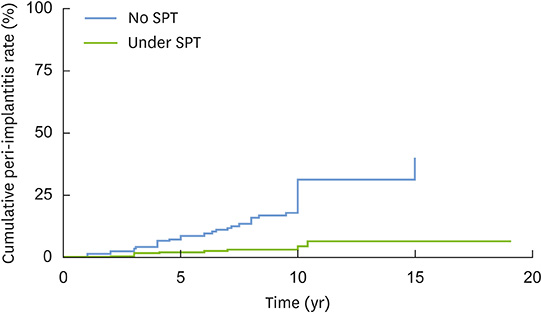
Figure 4 Cumulative peri-implantitis rate at the implant level in patients receiving SPT and those not receiving SPT over a 19-year follow-up period in the CP group estimated with the Kaplan-Meier method. SPT: supportive periodontal therapy, CP: current peri-implantitis.
Reference
-
1. Muddugangadhar BC, Amarnath GS, Sonika R, Chheda PS, Garg A. Meta-analysis of failure and survival rate of implant-supported single crowns, fixed partial denture, and implant tooth-supported prostheses. J Int Oral Health. 2015; 7:11–17.2. Jung RE, Zembic A, Pjetursson BE, Zwahlen M, Thoma DS. Systematic review of the survival rate and the incidence of biological, technical, and aesthetic complications of single crowns on implants reported in longitudinal studies with a mean follow-up of 5 years. Clin Oral Implants Res. 2012; 23:Suppl 6. 2–21.3. Pjetursson BE, Thoma D, Jung R, Zwahlen M, Zembic A. A systematic review of the survival and complication rates of implant-supported fixed dental prostheses (FDPs) after a mean observation period of at least 5 years. Clin Oral Implants Res. 2012; 23:Suppl 6. 22–38.
Article4. Albrektsson T, Isidor F. Consensus report of session IV. In : Lang NP, Karring T, editors. Proceedings of the 1st European Workshop on Periodontology. Chicago: Quintessence;1994. p. 365.5. Lindhe J, Meyle J. Group D of European Workshop on Periodontology. Peri-implant diseases: consensus report of the sixth European Workshop on Periodontology. J Clin Periodontol. 2008; 35:282–285.
Article6. Larsson L, Decker AM, Nibali L, Pilipchuk SP, Berglundh T, Giannobile WV. Regenerative medicine for periodontal and peri-implant diseases. J Dent Res. 2016; 95:255–266.
Article7. Fu JH, Wang HL. Can periimplantitis be treated? Dent Clin North Am. 2015; 59:951–980.
Article8. Derks J, Schaller D, Håkansson J, Wennström JL, Tomasi C, Berglundh T. Peri-implantitis - onset and pattern of progression. J Clin Periodontol. 2016; 43:383–388.
Article9. Albrektsson T, Canullo L, Cochran D, De Bruyn H. “Peri-implantitis”: a complication of a foreign body or a man-made “Disease”. Facts and fiction. Clin Implant Dent Relat Res. 2016; 18:840–849.
Article10. Derks J, Tomasi C. Peri-implant health and disease. A systematic review of current epidemiology. J Clin Periodontol. 2015; 42:Suppl 16. S158–S171.
Article11. Salvi GE, Cosgarea R, Sculean A. Prevalence and mechanisms of peri-implant diseases. J Dent Res. 2017; 96:31–37.
Article12. Eke PI, Dye BA, Wei L, Slade GD, Thornton-Evans GO, Borgnakke WS, et al. Update on prevalence of periodontitis in adults in the United States: NHANES 2009 to 2012. J Periodontol. 2015; 86:611–622.
Article13. Heitz-Mayfield LJ. Peri-implant diseases: diagnosis and risk indicators. J Clin Periodontol. 2008; 35:292–304.
Article14. Monje A, Galindo-Moreno P, Tözüm TF, Suárez-López del Amo F, Wang HL. Into the paradigm of local factors as contributors for peri-implant disease: short communication. Int J Oral Maxillofac Implants. 2016; 31:288–292.
Article15. Heitz-Mayfield LJ, Huynh-Ba G. History of treated periodontitis and smoking as risks for implant therapy. Int J Oral Maxillofac Implants. 2009; 24:Suppl. 39–68.16. Sgolastra F, Petrucci A, Severino M, Gatto R, Monaco A. Periodontitis, implant loss and peri-implantitis. A meta-analysis. Clin Oral Implants Res. 2015; 26:e8–16.
Article17. Monje A, Aranda L, Diaz KT, Alarcón MA, Bagramian RA, Wang HL, et al. Impact of maintenance therapy for the prevention of peri-implant diseases: a systematic review and meta-analysis. J Dent Res. 2016; 95:372–379.
Article18. Begg MD. Analysis of correlated responses. In : Lesaffre E, Feine J, Leroux B, Declerck D, editors. Statistical and methodological aspects of oral health research. Chichester: John Wiley & Sons;2009. p. 221–240.19. Albrektsson T, Chrcanovic B, Östman PO, Sennerby L. Initial and long-term crestal bone responses to modern dental implants. Periodontol 2000. 2017; 73:41–50.
Article20. Roccuzzo M, De Angelis N, Bonino L, Aglietta M. Ten-year results of a three-arm prospective cohort study on implants in periodontally compromised patients. Part 1: implant loss and radiographic bone loss. Clin Oral Implants Res. 2010; 21:490–496.
Article21. Chang M, Wennström JL. Bone alterations at implant-supported FDPs in relation to inter-unit distances: a 5-year radiographic study. Clin Oral Implants Res. 2010; 21:735–740.
Article22. Balshi TJ, Hernandez RE, Pryszlak MC, Rangert B. A comparative study of one implant versus two replacing a single molar. Int J Oral Maxillofac Implants. 1996; 11:372–378.
Article23. Jeong JS, Chang M. Food impaction and periodontal/peri-implant tissue conditions in relation to the embrasure dimensions between implant-supported fixed dental prostheses and adjacent teeth: a cross-sectional study. J Periodontol. 2015; 86:1314–1320.
Article24. Ebell MH, Siwek J, Weiss BD, Woolf SH, Susman JL, Ewigman B, et al. Simplifying the language of evidence to improve patient care: strength of recommendation taxonomy (SORT): a patient-centered approach to grading evidence in medical literature. J Fam Pract. 2004; 53:111–120.25. Blicher B, Joshipura K, Eke P. Validation of self-reported periodontal disease: a systematic review. J Dent Res. 2005; 84:881–890.
Article26. Eke PI, Dye BA, Wei L, Slade GD, Thornton-Evans GO, Beck JD, et al. Self-reported measures for surveillance of periodontitis. J Dent Res. 2013; 92:1041–1047.
Article27. Coli P, Christiaens V, Sennerby L, Bruyn H. Reliability of periodontal diagnostic tools for monitoring peri-implant health and disease. Periodontol 2000. 2017; 73:203–217.
Article28. Koldsland OC, Scheie AA, Aass AM. Prevalence of peri-implantitis related to severity of the disease with different degrees of bone loss. J Periodontol. 2010; 81:231–238.
Article29. Zetterqvist L, Feldman S, Rotter B, Vincenzi G, Wennström JL, Chierico A, et al. A prospective, multicenter, randomized-controlled 5-year study of hybrid and fully etched implants for the incidence of peri-implantitis. J Periodontol. 2010; 81:493–501.
Article30. Sanz M, Chapple IL. Working Group 4 of the VIII European Workshop on Periodontology. Clinical research on peri-implant diseases: consensus report of Working Group 4. J Clin Periodontol. 2012; 39:Suppl 12. 202–206.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Risk indicators for mucositis and peri-implantitis: results from a practice-based cross-sectional study
- Prevalence and risk factors of peri-implant mucositis and peri-implantitis after at least 7 years of loading
- Advanced peri-implantitis cases with radical surgical treatment
- Risk factors of peri-implantitis: a narrative review
- Biomarkers associated with periodontitis and peri-implantitis: a systematic review
