Perinatology.
2017 Jun;28(2):69-73. 10.14734/PN.2017.28.2.69.
Ileal Atresia Presenting with Massive Chylous Ascites and Hydrocele in a Newborn
- Affiliations
-
- 1Department of Pediatrics, Ewha Womans University School of Medicine, Seoul, Korea. sujin-cho@ewha.ac.kr
- 2Department of General Surgery, Ewha Womans University School of Medicine, Seoul, Korea.
- 3Department of Radiology, Ewha Womans University School of Medicine, Seoul, Korea.
- KMID: 2386355
- DOI: http://doi.org/10.14734/PN.2017.28.2.69
Abstract
- We report a case of ileal atresia presenting with massive chylous ascites and hydrocele in a neonate. A male neonate was born at 38 weeks of gestation with a weight of 3,360 grams. The antenatal ultrasonography performed at 37âºâ¶ weeks of gestation showed ascites and huge bilateral hydrocele. At birth, he manifested hypotonia, a massively distended abdomen and huge bilateral hydrocele. Exploratory laparotomy was performed on the day of birth. A large amount of chyle (approximately 200 mL) was found in the peritoneal cavity between the bowel loops. An additional 120 mL of chyle was removed from both scrotal sacs. The color of chyle was ivory yellow with whitish debris. Ileal atresia had occurred 7 cm above the ileocecal valve. The proximal small bowel was disconnected, and the distal small bowel loop ended in a blind loop. Lymphatic drainage from that cross section of the proximal small bowel might be a cause of chylous ascites. Segmental small bowel resection and double barrel ileostomy was performed. We described this case with a review of the literature.
Keyword
MeSH Terms
Figure
-

Fig. 1 The ascites depth of 2.3 cm was detected by antenatal ultrasonography.

Fig. 2 At birth, the patient showed a massively distended abdomen and huge bilateral hydrocele.
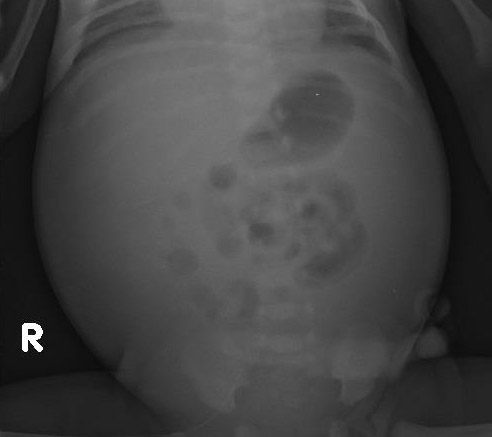
Fig. 3 On the abdomen x-ray, the bowel gas was located centrally.

Fig. 4 In the ultrasonography, large amount of ascites and thickening of the small bowel loop were seen.

Fig. 5 The proximal small bowel was disconnected, and the distal small bowel ended in a blind loop.

Fig. 6 Few necrotic tissues with scanty amount of viable small intestine wall were observed.
Reference
-
1. Held JM, Restrepo R, Ricca R. Chylous ascites in a neonate with hydrops fetalis. Am Surg. 2016; 82:783–784.
Article2. Mouravas V, Dede O, Hatziioannidis H, Spyridakis I, Filippopoulos A. Diagnosis and management of congenital neonatal chylous ascites. Hippokratia. 2012; 16:175–180.3. Nigam A, Kumar M, Gulati S. Fetal ascites and hydrometrocolpos due to persistent urogenital sinus and cloaca: a rare congenital anomaly and review of literature. BMJ Case Rep. 2014; 2014:bcr2013202231.
Article4. Baccega F, de Lourdes Brizot M, Jornada Krebs VL, Vieira Francisco RP, Zugaib M. Nonimmune fetal ascites: identification of ultrasound findings predictive of perinatal death. J Perinat Med. 2016; 44:195–200.
Article5. Moon SK, Kim JN, Choi MJ, Seo JS, Kim JS, Kim HY, et al. A case of chylous ascites secondary to congenital ileal atresia. Korean J Perinatol. 1997; 8:309–314.6. Virgone C, D'antonio F, Khalil A, Jonh R, Manzoli L, Giuliani S. Accuracy of prenatal ultrasound in detecting jejunal and ileal atresia: systematic review and meta-analysis. Ultrasound Obstet Gynecol. 2015; 45:523–529.
Article7. Chen HD, Jiang H, Kan A, Huang LE, Zhong ZH, Zhang ZC, et al. Intestinal obstruction due to dual gastrointestinal atresia in infants: diagnosis and management of 3 cases. BMC Gastroenterol. 2014; 14:108.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Chylous Ascites Secondary to Congenital Ileal Atresia
- Successful Treatment in a Newborn Infant with Chylous Ascites and Chylous Hydrocele
- A Case of Chylous Ascites in an Infant Boy
- A case of massive serous ascites following radical hysterectomy with bilateral pelvic lymphadenectomy for cervical adenocarcinoma stage IB2
- Umbilical Venous Catheter Complication Presenting as Chylous Ascites in a Newborn: Intraperitoneal Extravasation of Total Parenteral Nutrition Infusate
