Combined Use of Neutrophil to Lymphocyte Ratio and C-Reactive Protein Level to Predict Clinical Outcomes in Acute Myocardial Infarction Patients Undergoing Percutaneous Coronary Intervention
- Affiliations
-
- 1Department of Internal Medicine, Busan Paik Hospital, Inje University College of Medicine, Busan, Korea. jsjang71@gmail.com
- KMID: 2385393
- DOI: http://doi.org/10.4070/kcj.2016.0327
Abstract
- BACKGROUND AND OBJECTIVES
Both neutrophil to lymphocyte ratio (NLR) and C-reactive protein (CRP) are biomarkers associated with poor prognosis of patients with acute myocardial infarction (AMI). However, the combined usefulness of NLR and CRP in predicting adverse outcomes has not been investigated.
SUBJECTS AND METHODS
We analyzed 381 consecutive AMI patients who underwent percutaneous coronary intervention (PCI) from January 2012 to January 2014. The endpoints were all-cause mortality, recurrent myocardial infarction (MI), stent thrombosis, repeat revascularization, stroke, and major adverse cardiac and cerebrovascular events (MACCE) at 2-year follow-up. Included patients were divided into 4 groups according to the optimal cut-off values for NLR and CRP on receiver operating characteristic analysis predicting mortality.
RESULTS
Patients with both high NLR (>6.30) and high CRP (>0.76) had significantly greater risk of all-cause death and MACCE at 24 months, with no significant increase in the risk of recurrent MI, stent thrombosis, or stroke compared with patients with either low NLR or low CRP, as well as those with low NLR and low CRP. Kaplan-Meier analysis revealed significantly lower survival in patients with high NLR-CRP. On Cox multivariate analysis, high NLR-CRP (hazard ratio 23.172, 95% confidence interval 6.575 to 81.671, p<0.001) was an independent predictor of all-cause death.
CONCLUSION
Elevated levels of both NLR and CRP are associated with increased risk of long-term mortality in AMI patients who have undergone PCI.
Keyword
MeSH Terms
Figure
-
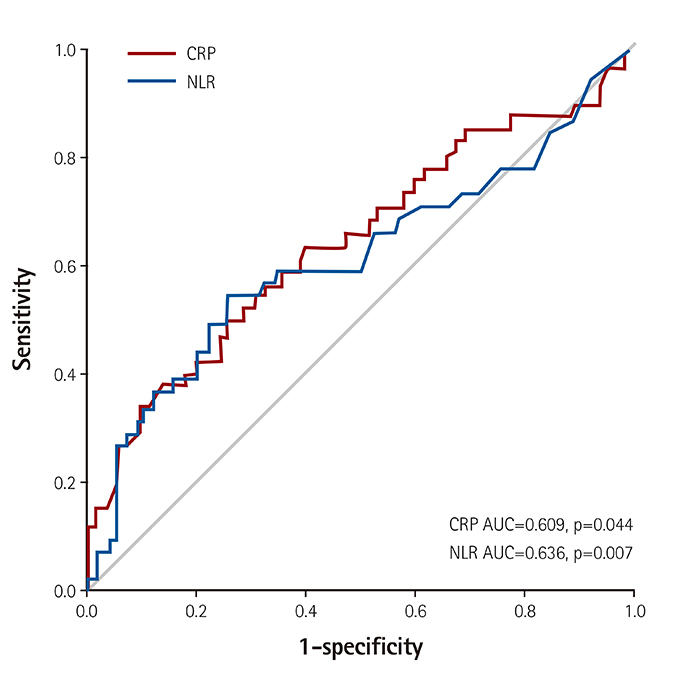
Fig. 1 ROC curves of CRP and NLR according to 24 month all-cause death. CRP: C-reactive protein, NLR: neutrophil-to-lymphocyte ratio, AUC: area under the receiver operator characteristic curve, ROC: receiver operator characteristic, MACCE: major adverse cardiac and cerebrovascular events.
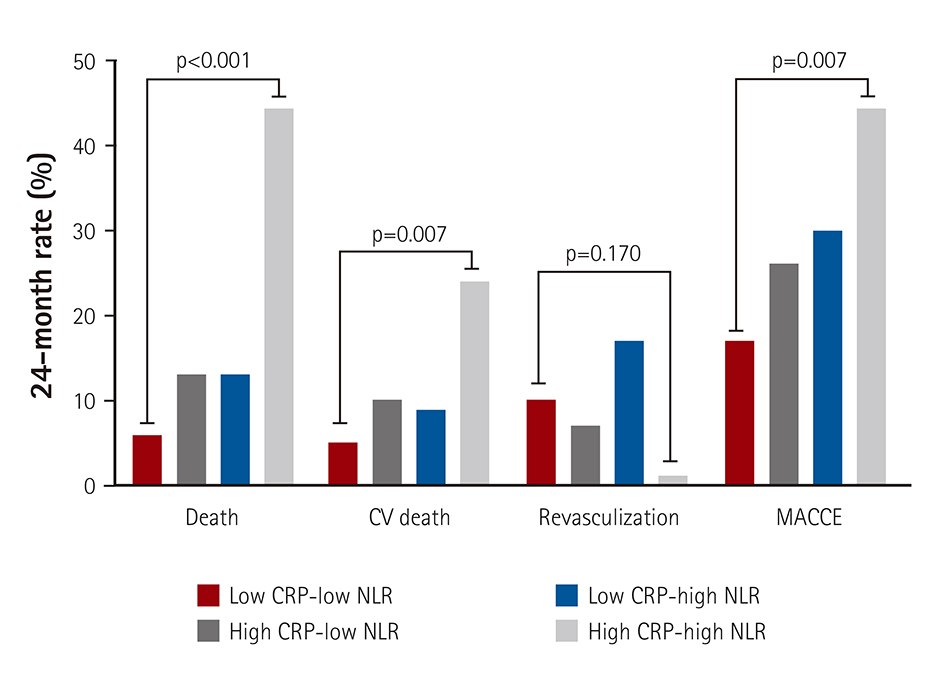
Fig. 2 Clinical outcomes in 4 groups at 24 months. Patients in the high NLR and high CRP group had significantly higher rates of all-cause mortality, cardiovascular mortality, and MACCE. The p values were compared between the low NLR-low CRP group and the high NLR-high CRP group. CV: cardiovascular, CRP: C-reactive protein, NLR: neutrophil-to-lymphocyte ratio, MACCE: major adverse cardiac and cerebrovascular events.
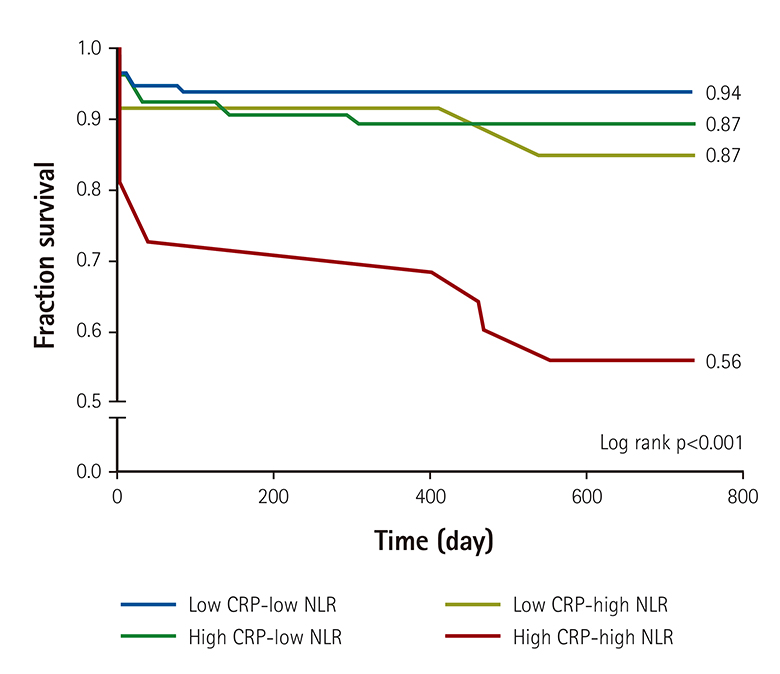
Fig. 3 Kaplan-Meier survival curve of 24 month all-cause death. Patients in the high NLR-high CRP group showed the lowest 24-month death-free survival of all groups. CRP: C-reactive protein, NLR: neutrophil-to-lymphocyte ratio.
Reference
-
1. Ross R. Atherosclerosis--an inflammatory disease. N Engl J Med. 1999; 340:115–126.2. Libby P, Ridker PM, Hansson GK. Leducq Transatlantic Network on Atherothrombosis. Inflammation in atherosclerosis: from pathophysiology to practice. J Am Coll Cardiol. 2009; 54:2129–2138.3. Ogita M, Miyauchi K, Tsuboi S, et al. Impact of combined C-reactive protein and high-density lipoprotein cholesterol levels on long-term outcomes in patients with coronary artery disease after a first percutaneous coronary intervention. Am J Cardiol. 2015; 116:999–1002.4. Han YC, Yang TH, Kim DI, et al. Neutrophil to lymphocyte ratio predicts long-term clinical outcomes in patients with ST-segment elevation myocardial infarction undergoing primary percutaneous coronary intervention. Korean Circ J. 2013; 43:93–99.5. Gibson PH, Croal BL, Cuthbertson BH, et al. Preoperative neutrophil-lymphocyte ratio and outcome from coronary artery bypass grafting. Am Heart J. 2007; 154:995–1002.6. Gibson PH, Cuthbertson BH, Croal BL, et al. Usefulness of neutrophil/lymphocyte ratio as predictor of new-onset atrial fibrillation after coronary artery bypass grafting. Am J Cardiol. 2010; 105:186–191.7. Nakamura T, Matsumine A, Matsubara T, Asanuma K, Uchida A, Sudo A. The combined use of the neutrophil-lymphocyte ratio and C-reactive protein level as prognostic predictors in adult patients with soft tissue sarcoma. J Surg Oncol. 2013; 108:481–485.8. O'Gara PT, Kushner FG, Ascheim DD, et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association task force on practice guidelines. Circulation. 2013; 127:e362–e425.9. Amsterdam EA, Wenger NK, Brindis RG, et al. 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes: a report of the American College of Cardiology/American Heart Association task force on practice guidelines. J Am Coll Cardiol. 2014; 64:e139–e228.10. Cutlip DE, Windecker S, Mehran R, et al. Clinical end points in coronary stent trials: a case for standardized definitions. Circulation. 2007; 115:2344–2351.11. Azab B, Zaher M, Weiserbs KF, et al. Usefulness of neutrophil to lymphocyte ratio in predicting short- and long-term mortality after non-ST-elevation myocardial infarction. Am J Cardiol. 2010; 106:470–476.12. Tamhane UU, Aneja S, Montgomery D, Rogers EK, Eagle KA, Gurm HS. Association between admission neutrophil to lymphocyte ratio and outcomes in patients with acute coronary syndrome. Am J Cardiol. 2008; 102:653–657.13. Fowler AJ, Agha RA. Neutrophil/lymphocyte ratio is related to the severity of coronary artery disease and clinical outcome in patients undergoing angiography--the growing versatility of NLR. Atherosclerosis. 2013; 228:44–45.14. Keeley EC, Boura JA, Grines CL. Primary angioplasty versus intravenous thrombolytic therapy for acute myocardial infarction: a quantitative review of 23 randomised trials. Lancet. 2003; 361:13–20.15. Forman MB, Puett DW, Virmani R. Endothelial and myocardial injury during ischemia and reperfusion: pathogenesis and therapeutic implications. J Am Coll Cardiol. 1989; 13:450–459.16. Alpert JS, Thygesen K, Antman E, Bassand JP. Myocardial infarction redefined--a consensus document of the joint european society of cardiology/american college of cardiology committee for the redefinition of myocardial infarction. J Am Coll Cardiol. 2000; 36:959–969.17. De Servi S, Mariani M, Mariani G, Mazzone A. C-reactive protein increase in unstable coronary disease cause or effect? J Am Coll Cardiol. 2005; 46:1496–1502.18. Hansson GK, Libby P, Tabas I. Inflammation and plaque vulnerability. J Intern Med. 2015; 278:483–493.19. Agrawal A, Gang TB, Rusiñol AE. Recognition functions of pentameric C-reactive protein in cardiovascular disease. Mediators Inflamm. 2014; 2014:319215.20. Deftereos S, Giannopoulos G, Angelidis C, et al. Anti-inflammatory treatment with colchicine in acute myocardial infarction: a pilot study. Circulation. 2015; 132:1395–1403.21. Ugur M, Gul M, Bozbay M, et al. The relationship between platelet to lymphocyte ratio and the clinical outcomes in ST elevation myocardial infarction underwent primary coronary intervention. Blood Coagul Fibrinolysis. 2014; 25:806–811.22. Temiz A, Gazi E, Güngör Ö, et al. Platelet/lymphocyte ratio and risk of in-hospital mortality in patients with ST-elevated myocardial infarction. Med Sci Monit. 2014; 20:660–665.23. Sari I, Sunbul M, Mammadov C, et al. Relation of neutrophil-tolymphocyte and platelet-to-lymphocyte ratio with coronary artery disease severity in patients undergoing coronary angiography. Kardiol Pol. 2015; 73:1310–1316.24. Cho KI, Ann SH, Singh GB, Her AY, Shin ES. Combined usefulness of the platelet-to-lymphocyte ratio and the neutrophil-to-lymphocyte ratio in predicting the long-term adverse events in patients who have undergone percutaneous coronary intervention with a drug-eluting stent. PLoS One. 2015; 10:e0133934.25. Helmers C. Short and long-term prognostic indices in acute myocardial infarction. A study of 606 patients initially treated in a coronary care unit. Acta Med Scand Suppl. 1973; 555:7–26.26. Kelly TL, Gilpin E, Ahnve S, Henning H, Ross J Jr. Smoking status at the time of acute myocardial infarction and subsequent prognosis. Am Heart J. 1985; 110:535–541.27. Sparrow D, Dawber TR. The influence of cigarette smoking on prognosis after a first myocardial infarction. A report from the Framingham study. J Chronic Dis. 1978; 31:425–432.28. Weinblatt E, Shapiro S, Frank CW, Sager RV. Prognosis of men after first myocardial infarction: mortality and first recurrence in relation to selected parameters. Am J Public Health Nations Health. 1968; 58:1329–1347.29. Aune E, Røislien J, Mathisen M, Thelle DS, Otterstad JE. The “smoker's paradox” in patients with acute coronary syndrome: a systematic review. BMC Med. 2011; 9:97.30. Misumida N, Kobayashi A, Kanei Y. Racial differences in the neutrophil-to-lymphocyte ratio in patients with non-ST-segment elevation myocardial infarction. Coron Artery Dis. 2015; 26:381–385.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- No-Reflow Phoenomenon by Intracoronary Thrombus in Acute Myocardial Infarction
- Acute myocardial infarction in young patient probably due to Kawasaki disease
- Neutrophil to Lymphocyte Ratio Predicts Long-Term Clinical Outcomes in Patients with ST-Segment Elevation Myocardial Infarction Undergoing Primary Percutaneous Coronary Intervention
- Cardiac arrest due to an unexpected acute myocardial infarction during head and neck surgery: A case report
- Clinical outcome in elderly patients older than 70 years with acute myocardial infarction after use of platelet glycoprotein IIb/IIIa receptor blocker during percutaneous coronary intervention: Comparison with those younger than 70 years
