Corticospinal Tract and Pontocerebellar Fiber of Central Pontine Myelinolysis
- Affiliations
-
- 1Department of Physical Medicine and Rehabilitation, Institute for Medical Sciences, Chonbuk National University Medical School, Research Institute of Clinical Medicine, Chonbuk National University Hospital, Jeonju 561-180, Korea. shpark0130@jbnu.ac.kr
- 2Department of Radiology, Institute for Medical Sciences, Chonbuk National University Medical School, Research Institute of Clinical Medicine, Chonbuk National University Hospital, Jeonju 561-180, Korea.
Abstract
- Central pontine myelinolysis is a rare neurologic disorder that is defined by demyelination of longitudinally descending tracts and transversly crossing fibers in the basis pontis. Frequently observed clinical manifestations of this disorder include sudden weakness, dysphagia, loss of consciouness and locked-in syndrome. However, there have been a few studies that reported a benign course of this disease, which include cerebellar signs, such as ataxia, intention tremor, and dysarthria. Here we report on a 53-year-old male with a history of liver cirrhosis who showed the cerebellar type of central pontine myelinolysis. The patient was diagnosed with central pontine myelinolysis based on clinical presentations and magnetic resonance imaging findings after a liver transplantation. Conventional magenetic resonance imaging (MRI) revealed the preservation of the corticospinal tract and abnormal pontocerebellar fibers. However, these findings were not sufficient to define the pathophysiology of our patient. Electrophysiologic analysis and diffusion tensor imaging (DTI) were performed to investigate cerebellar signs in this case. Delayed central motor conduction time (CMCT) to the tibialis anterior muscle with transcranial magnetic stimulation (TMS) was observed, which indicated demyelination of the corticospinal tract. Also, diffusion tensor imaging showed abnormal pontocerebellar fibers, which might have been caused by cerebellar dysfunction in our patient. A combination of TMS and DTI was also used to determine the pathophysiology of this disease.
Keyword
MeSH Terms
-
Ataxia
Cerebellar Diseases
Deglutition Disorders
Demyelinating Diseases
Diffusion Tensor Imaging
Dysarthria
Humans
Liver Cirrhosis
Liver Transplantation
Magnetic Resonance Imaging
Male
Muscles
Myelinolysis, Central Pontine
Nervous System Diseases
Pyramidal Tracts
Quadriplegia
Transcranial Magnetic Stimulation
Tremor
Figure
-
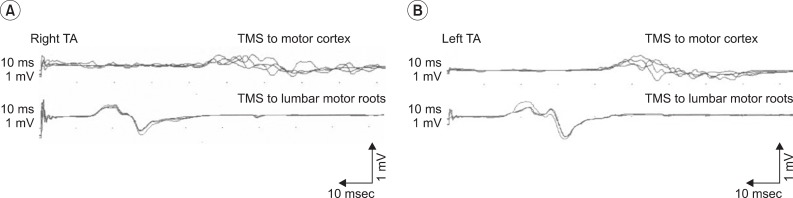
Fig. 1 The recordings are the right TA (A) and left TA (B) motor evoked potential responses to the TMS of the motor cortex and those to the TMS of the lumbar motor roots. Each trace consists of four superimposed traces. Longer latencies of bilateral motor evoked potentials in TMS to motor cortex are observed. TMS: Transcranial magnetic stimulation, TA: Tibialis anterior muscle.
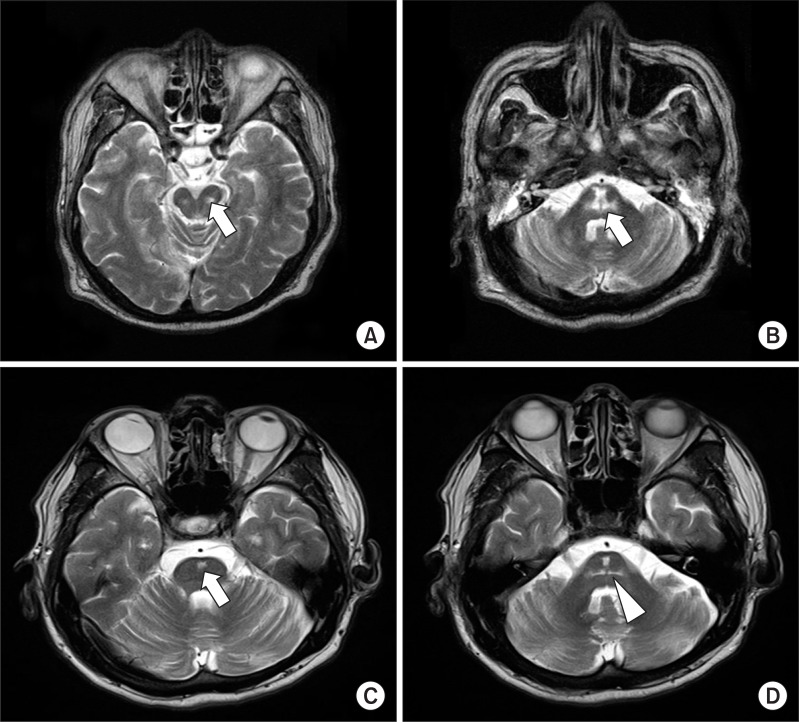
Fig. 2 The image of axial fast spin echo T2 -weighted images show a bilateral symmetrical hyperintense lesion (arrow on A, B) with a spared corticospinal tract at the midbrain (A) and pons (B) at onset. After 5 years, an oval cavitary lesion (arrow on C) at the center of the basis pontis was observed. The pons is mildly atrophic, and there are bilateral symmetrical linear lesions (arrowhead on D) that indicate pontocerebellar fibers.

Fig. 3 To evaluate the pontocerebellar fiber (arrow on A) in the Diffusion tensor images, Fractional anisotropy and the Apparent diffusion coefficient was measured in a region of interest located on the Middle cerebellar peduncle in the coronal section (arrowhead on B).
Reference
-
1. Yu J, Zheng SS, Liang TB, Shen Y, Wang WL, Ke QH. Possible causes of central pontine myelinolysis after liver transplantation. World J Gastroenterol. 2004; 10:2540–2543. PMID: 15300900.
Article2. Laubenberger J, Schneider B, Ansorge O, Götz F, Häussinger D, Volk B, Langer M. Central pontine myelinolysis: clinical presentation and radiologic findings. Eur Radiol. 1996; 6:177–183. PMID: 8797975.
Article3. Bassetti C, Mathis J, Hess CW. Multimodal electrophysiological studies including motor evoked potentials in patients with locked-in syndrome: report of six patients. J Neurol Neurosurg Psychiatry. 1994; 57:1403–1406. PMID: 7964820.
Article4. Kim J, Lee SK, Lee JD, Kim YW, Kim DI. Decreased fractional anisotropy of middle cerebellar peduncle in crossed cerebellar diaschisis: diffusion-tensor imaging-positron-emission tomography correlation study. Am J Neuroradiol. 2005; 26:2224–2228. PMID: 16219826.5. Taoka T, Kin T, Nakagawa H, Hirano M, Sakamoto M, Wada T, Takayama K, Wuttikul C, Iwasaki S, Ueno S, et al. Diffusivity and diffusion anisotropy of cerebellar peduncles in cases of spinocerebellar degenerative disease. NeuroImage. 2007; 37:387–393. PMID: 17583535.
Article6. Lilje CG, Heinen F, Laubenberger J, Krug I, Brandis M. Benign course of central pontine myelionlysis in a patient with anorexia nervosa. Pediatr Neurol. 2002; 27:132–135. PMID: 12213614.7. Schmahmann JD, Ko R, MacMore J. The human basis pontis: motor syndromes and topographic organization. Brain. 2004; 127:1269–1291. PMID: 15128614.
Article8. Garzon T, Mellibovsky L, Roquer J, Perich X, Diez-Perez A. Ataxic form of central pontine myelinolysis. Lancet Neurol. 2002; 1:517–518. PMID: 12849338.
Article9. Kim EJ, Oh SY, Choi HC, Lim MH, Shin BS. Central pontine myelinolysis presenting with cerebellar ataxia. J Korean Neurol Assoc. 2009; 27:264–267.10. De Simone T, Regna-Gladin C, Carriero MR, Farina L, Savoiardo M. Wallerian degeneration of the pontocerebellar fibers. Am J Neuroradiol. 2005; 26:1062–1065. PMID: 15891160.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A case of central pontine and extrapontine myelinolysis with early hypermetabolism on 18FDG-PET scan
- Central Pontine and Extrapontine Myelinolysis in a Patient with Traumatic Brain Injury Following Not Rapid Correction of Hyponatremia: A Case Report
- A Case of Subacute Onset Choreoathetosis as Sequelae of Central Pontine and Extrapontine Myelinolysis
- Neuropsychological Findings of Extrapontine Myelinolysis without Central Pontine Myelinolysis: Initial and Follow-up Evaluation
- A Case of Central Pontine Myelinolysis Associated with Hypokalemia in Hyperemesis Gravidarum
