Actinomycosis Involving Chronic Pancreatitis: A Case Report with Literature Review
- Affiliations
-
- 1Department of Internal Medicine, Kyungpook National University School of Medicine, Daegu, Korea. cmcho@knu.ac.kr
- 2Department of Radiology, Kyungpook National University School of Medicine, Daegu, Korea.
- 3Department of Pathology, Kyungpook National University School of Medicine, Daegu, Korea.
- KMID: 2383414
- DOI: http://doi.org/10.4166/kjg.2017.69.3.191
Abstract
- Actinomycosis is a slowly progressive, chronic infectious disease. It is caused by the genus Actinomyces, which are gram-positive anaerobic bacteria. It presents as a mass-like lesion, composed of bacterial nidus and characteristic granulomatous inflammatory fibrosis. As such, it has frequently been mistaken for a malignancy. Surgical resection is a common procedure in these patients prior to a definite diagnosis. Although actinomycosis can occur in a variety of regions, including oral-cervicofacial, thoracic, and abdominopelvic cavities, the involvement of the pancreas is very rare. We report a case of a 44-year-old male with a symptomatic actinomycosis caused by a mass in the tail of the pancreas. The diagnosis was made using an endoscopic ultrasound-guided fine needle aspiration biopsy without surgical resection. After the treatment with antibiotics, the pancreatic mass was confirmed to be resolved on the follow-up computed tomography.
Keyword
MeSH Terms
Figure
-

Fig. 1. Computed tomography scan images. (A) Multiple calcifications and stones (black arrows) were also noted in the head of the pancreas. (B) Contrast-enhanced axial image (portal phase) revealed diffuse parenchymal swelling with multiple calcification (black arrows) at the body of the pancreas. (C) Contrast-enhanced coronal image (portal phase) showed heterogeneous enhancement of the pancreas parenchyma and peripancreatic strands (white arrows). (D) Multifocal uneven pancreatic duct dilation (white asterisk) was also observed.

Fig. 2. Endoscopic ultrasonography (EUS) images. (A) A 19-mm sized, ill-defined, hypoechoic and heterogenous mass with central calcification was identified at the pancreatic tail. (B) EUS-guided fine needle aspiration biopsy using a 20-gauge needle was performed.

Fig. 3. Microscopic findings for the specimen. The specimen revealed sulfur granules, consisting of a conglomeration of filamentous bacteria, which was shown at the surrounding tissue with dense inflammatory infiltration by lymphocytes, neutrophils, and foamy macrophages (A, hematoxylin and eosin stain, ×100; B, hematoxylin and eosin stain, ×400).
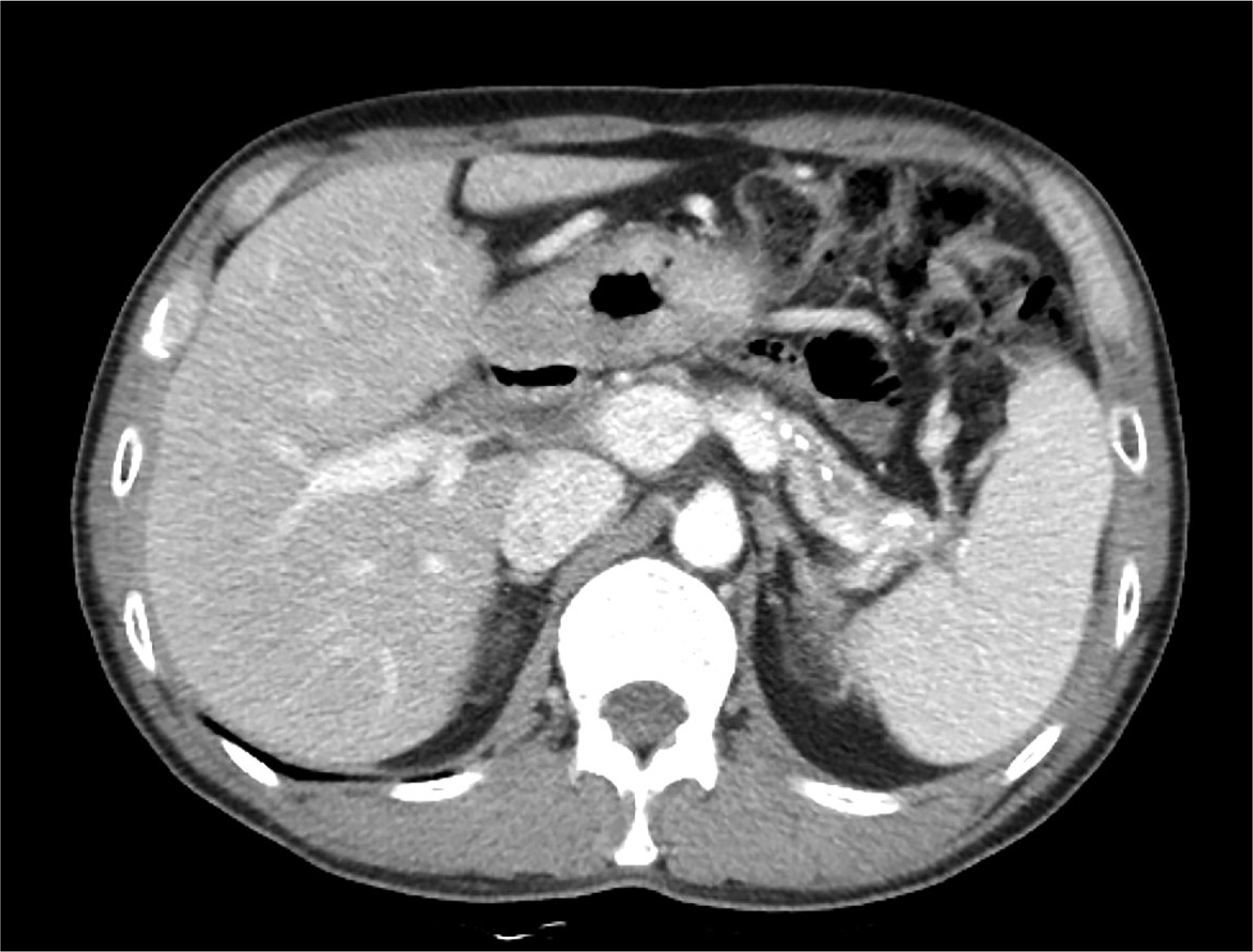
Fig. 4. Computed tomography image. Contrast-enhanced axial image (portal phase) revealed remarkable regression of pancreatic inflammatory swelling and peripancreatic inflammatory infiltration.
Reference
-
References
1. Wong VK, Turmezei TD, Weston VC. Actinomycosis. BMJ. 2011; 343:d6099.
Article2. Garner JP, Macdonald M, Kumar PK. Abdominal actinomycosis. Int J Surg. 2007; 5:441–448.
Article3. Kim MC, Lee H, Park J, et al. A solitary pancreatic actinomycosis mimicking pancreatic cancer. Korean J Pancreas Biliary Tract. 2015; 20:130–135.
Article4. Lee JH, Lee KG, Oh YH, Park HK, Lee KS. Actinomycosis of the pancreas: a case report and review of the literature. Hepatogastroenterology. 2010; 57:358–361.5. Maestro S, Trujillo R, Geneux K, et al. Pancreatic actinomycosis presenting as pancreatic mass and diagnosed with endoscopic ultrasound fine needle aspiration (EUS-FNA). Endoscopy. 2013; 45(Suppl 2 UCTN):E276–E277.
Article6. Piper MH, Schaberg DR, Ross JM, Shartsis JM, Orzechowski RW. Endoscopic detection and therapy of colonic actinomycosis. Am J Gastroenterol. 1992; 87:1040–1042.7. Harsch IA, Benninger J, Niedobitek G, et al. Abdominal actinomycosis: complication of endoscopic stenting in chronic pancreatitis? Endoscopy. 2001; 33:1065–1069.
Article8. Kuesters S, Timme S, Keck T. Uncommon cause of an inflammatory pancreatic head tumor. Diagnosis: purulent actinomycosis and incidental T1-carcinoid of the pancreatic head. Gastroenterology. 2011; 141:e9–e10.9. Somsouk M, Shergill AK, Grenert JP, Harris H, Cello JP, Shah JN. Actinomycosis mimicking a pancreatic head neoplasm diagnosed by EUS-guided FNA. Gastrointest Endosc. 2008; 68:186–187.
Article10. Hsu JT, Lo HC, Jan YY, Chen HM. Actinomycosis mimicking recurrent carcinoma after whipple's operation. World J Gastroenterol. 2005; 11:1722–1724.
Article11. Harris LA, DeCosse JJ, Dannenberg A. Abdominal actinomycosis: evaluation by computed tomography. Am J Gastroenterol. 1989; 84:198–200.12. Lee IJ, Ha HK, Park CM, et al. Abdominopelvic actinomycosis involving the gastrointestinal tract: CT features. Radiology. 2001; 220:76–80.
Article13. Cintron JR, Del Pino A, Duarte B, Wood D. Abdominal actinomycosis. Dis Colon Rectum. 1996; 39:105–108.
Article14. Ferrari TC, Couto CA, Murta-Oliveira C, Conceição SA, Silva RG. Actinomycosis of the colon: a rare form of presentation. Scand J Gastroenterol. 2000; 35:108–109.15. Weese WC, Smith IM. A study of 57 cases of actinomycosis over a 36-year period. A diagnostic ‘failure’ with good prognosis after treatment. Arch Intern Med. 1975; 135:1562–1568.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Actinomycosis of the Vocal Cord
- Middle Ear Actinomycosis Involving Facial Nerve and Lateral Semicircular Canal
- A Case of Pelvic Actinomycosis Associated with Intrauterine Contraceptive Device
- Acute Pancreatitis Complicating Spontaneous Acute Exacerbation of Chronic Hepatitis B Virus Infection: Case Report and Review of the Literature
- MR Findings of Hepatic Actinomycosis: Case Report
