Pancreatic Lymphoepithelial Cysts Diagnosed with Endosonography-guided Fine Needle Aspiration
- Affiliations
-
- 1Department of Internal Medicine, Chungbuk National University College of Medicine, Cheongju, Korea. smpark@chungbuk.ac.kr
- 2Department of Pathology, Chungbuk National University College of Medicine, Cheongju, Korea.
- 3Department of Radiology, Chungbuk National University College of Medicine, Cheongju, Korea.
- KMID: 2383405
- DOI: http://doi.org/10.4166/kjg.2017.69.4.253
Abstract
- Although lymphoepithelial cysts (LECs) of the pancreas are benign lesions, most of them have been treated with surgical resection due to diagnostic difficulty. We report a 66-year-old woman diagnosed with pancreatic LECs. Abdominal ultrasound revealed two masses in the pancreas, which were not visible on the abdominal computed tomography. In an abdominal magnetic resonance imaging, pancreas lesions showed solid tumors, which revealed a low signal intensity on T1-, moderate high signal intensity on T2 weighted images, and homogeneous delayed enhancement in the portal venous phase. Endosonography (EUS) revealed two hypoechoic round masses measuring 1.5 cm and 4.5 cm in the body and tail of the pancreas, respectively. EUS-guided fine needle aspiration (FNA) revealed squamous cells, amorphous keratinous debris, and lymphocytes. The patient was diagnosed with LECs of the pancreas. For the duration of the follow-up period of two years, imaging studies were unchanged. EUS-FNA is useful in making a definite diagnosis and avoiding unnecessary surgery. This is the first case of pancreatic LECs diagnosed with EUS-FNA in Korea.
MeSH Terms
Figure
-

Fig. 1. Abdominal ultrasonography revealing approximately 1.2 cm and 1.6 cm sized low echoic round lesions (arrows).

Fig. 2. Axial contrastenhanced abdominal computed tomography image showing no evidence of abnormal lesions and a normal pancreatic duct (A, B, arterial phase; C, D, delayed phase).
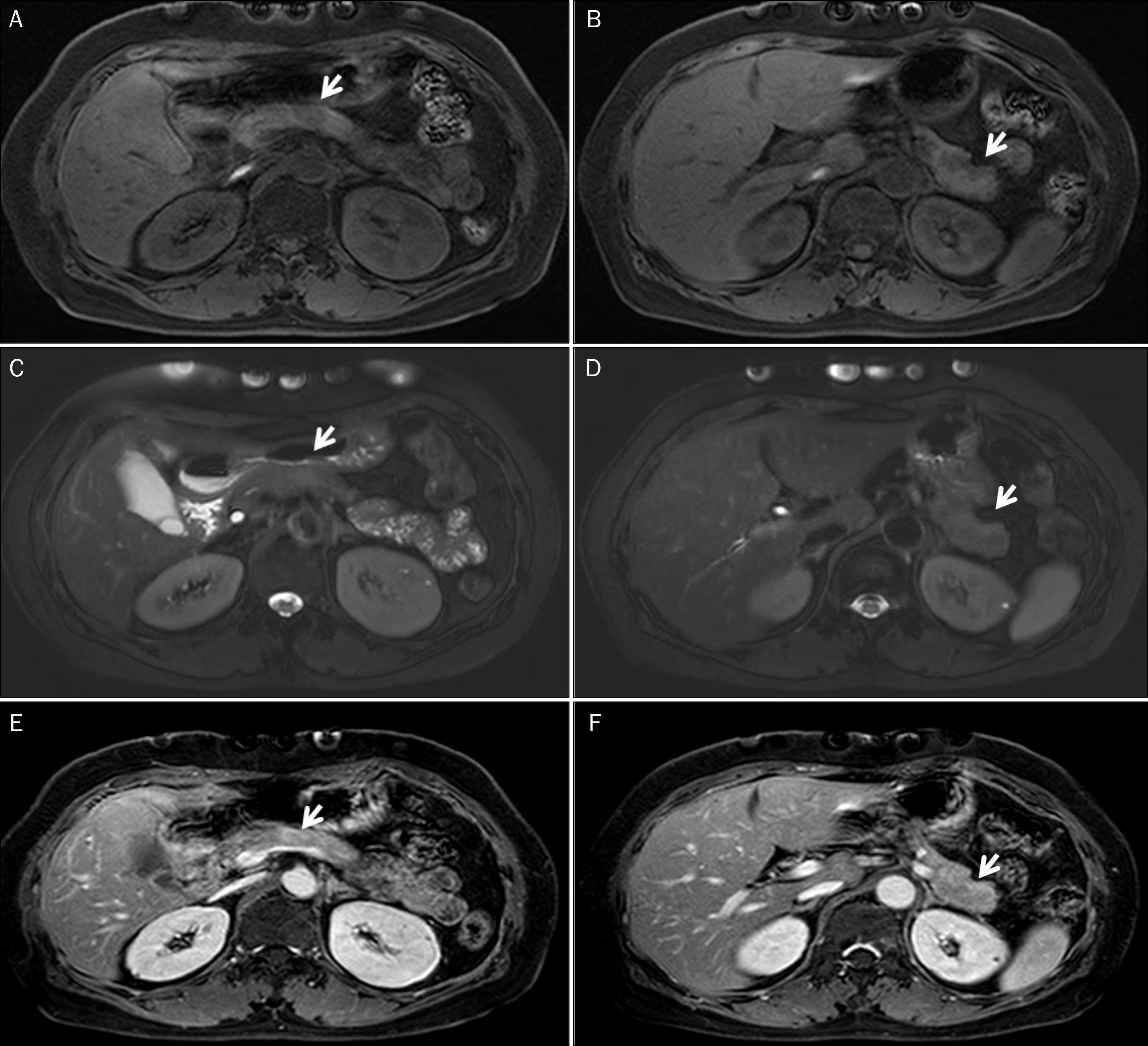
Fig. 3. Abdominal magnetic resonance images. Pre-contrast T1 weighted axial magnetic resonance images showing hypointense masses, 1.5 cm (A, arrow) and 4.5 cm (B, arrow) sized round shapes in the body and tail of the pancreas, respectively. They show moderate high signal intensity on T2 weighted images (C, D) and homogeneous delayed enhancement in the portal venous phase after contrast enhancement (E, F), suggesting solid tumors (arrows).
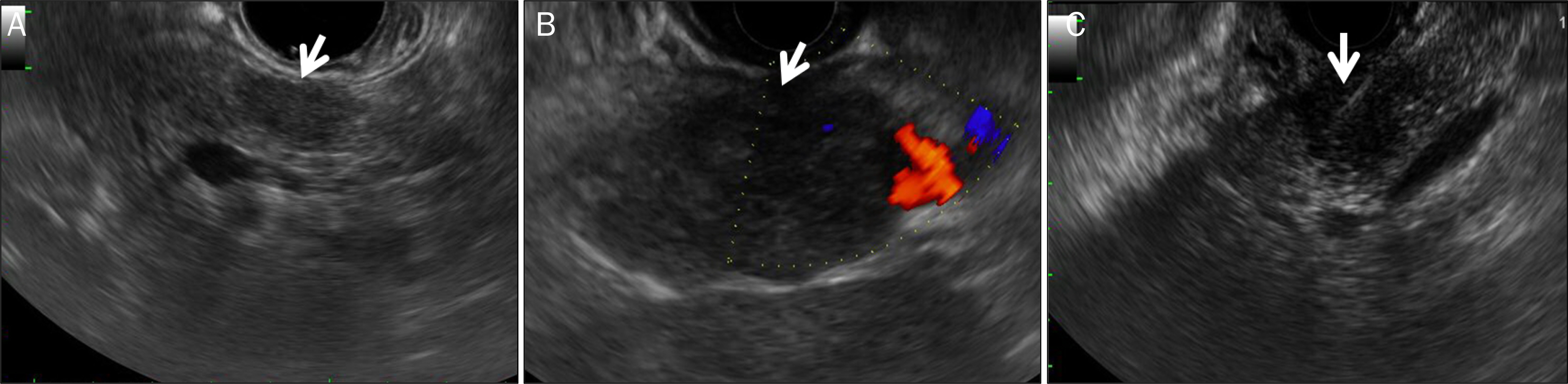
Fig. 4. Endosonography images. Radial endosonography revealing 1.5 cm (A, arrow) and 4.5 cm (B, arrow) sized hypoechoic, well-demarked, and round lesions in the body and tail of the pancreas, respectively. (C, arrow) Endosonography-guided fine needle aspiration using 22G needle.

Fig. 5. Cytologic smear obtained with two rounds of endosonography-guided fine needle aspiration (A and B obtained from 1st exam; C and D obtained from 2nd exam). Viable benign squamous cells (arrows) with lymphoid tissues (arrowheads) were seen, which were suggestive of lymphoepithelial cyst (Papanicolaou stain; A, ×200; B, C, ×400; D, ×1,000).
Reference
-
References
1. Lüchtrath H, Schriefers KH. A pancreatic cyst with features of a so-called branchiogenic cyst. Pathologe. 1985; 6:217–219.2. Truong LD, Rangdaeng S, Jordan PH Jr. Lymphoepithelial cyst of the pancreas. Am J Surg Pathol. 1987; 11:899–903.
Article3. Terakawa H, Makino I, Nakagawara H, et al. Clinical and radiological feature of lymphoepithelial cyst of the pancreas. World J Gastroenterol. 2014; 20:17247–17253.
Article4. Adsay NV, Hasteh F, Cheng JD, et al. Lymphoepithelial cysts of the pancreas: a report of 12 cases and a review of the literature. Mod Pathol. 2002; 15:492–501.
Article5. Dalal KS, DeWitt JM, Sherman S, Cramer HM, Tirkes T, Al-Haddad MA. Endoscopic ultrasound characteristics of pancreatic lymphoepithelial cysts: a case series from a large referral center. Endosc Ultrasound. 2016; 5:248–253.
Article6. Mege D, Grégoire E, Barbier L, Del Grande J, Le Treut YP. Lymphoepithelial cyst of the pancreas: an analysis of 117 patients. Pancreas. 2014; 43:987–995.7. Barbaros U, Erbil Y, Kapran Y, Bozbora A, Ozarmagan S, Bilgiç B. Lymphoepithelial cyst: a rare cystic tumor of the pancreas which mimics carcinoma. JOP. 2004; 5:392–394.8. Osiro S, Rodriguez JR, Tiwari KJ, et al. Is preoperative diagnosis possible? A clinical and radiological review of lymphoepithelial cysts of the pancreas. JOP. 2013; 14:15–20.9. Nasr J, Sanders M, Fasanella K, Khalid A, McGrath K. Lymphoepithelial cysts of the pancreas: an EUS case series. Gastrointest Endosc. 2008; 68:170–173.
Article10. Gao W, Masuda A, Matsumoto I, et al. A case of lymphoepithelial cyst of pancreas with unique "cheerios-like" appearance in EUS. Clin J Gastroenterol. 2012; 5:388–392.
Article11. Matrone A, Russo M, Mollica C, et al. Lymphoepithelial pancreatic cyst: an atypical benign pancreatic mass presenting with a “cheerios-like” appearance. JOP. 2010; 11:170–172.12. Matsubayashi H, Aikawa Y, Sugiura T, Sasaki K, Hotta K, Ono H. Pancreatic lymphoepithelial cyst showing multiple floating ball-like appearances. J Gastrointestin Liver Dis. 2016; 25:239–242.
Article13. VandenBussche CJ, Maleki Z. Fine-needle aspiration of squamous-lined cysts of the pancreas. Diagn Cytopathol. 2014; 42:592–599.
Article14. Martin J, Roberts KJ, Sheridan M, et al. Lymphoepithelial cysts of the pancreas: a management dilemma. Hepatobiliary Pancreat Dis Int. 2014; 13:539–544.
Article15. Kubo T, Takeshita T, Shimono T, Hashimoto S, Miki Y. Squamous-lined cyst of the pancreas: radiological-pathological correlation. Clin Radiol. 2014; 69:880–886.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Endoscopic Ultrasound-Guided Fine Needle Aspiration in Cystic Pancreatic Lesions
- Role of Repeated Endoscopic Ultrasound-Guided Fine Needle Aspiration for Inconclusive Initial Cytology Result
- Endoscopic Ultrasound-Guided Direct Intervention for Solid Pancreatic Tumors
- Endoscopic Ultrasound-Fine Needle Aspiration versus Core Biopsy for the Diagnosis of Subepithelial Tumors
- Lymphoepithelial cyst of the pancreas: A case report
