Post and core build-ups in crown and bridge abutments: Bio-mechanical advantages and disadvantages
- Affiliations
-
- 1Sunbeam Dental - General Dentistry, Manalapan, NJ, USA. mamounjo@gmail.com
- KMID: 2382611
- DOI: http://doi.org/10.4047/jap.2017.9.3.232
Abstract
- Dentists often place post and core buildups on endodontically treated abutments for crown and bridge restorations. This article analyzes the bio-mechanical purposes, advantages and disadvantages of placing a core or a post and core in an endodontically treated tooth and reviews literature on post and core biomechanics. The author assesses the scientific rationale of the claim that the main purpose of a post is to retain a core, or the claim that posts weaken teeth. More likely, the main function of a post is to help prevent the abutment, on which a crown is cemented, from fracturing such that the abutment separates from the tooth root, at a fracture plane that is located approximately and theoretically at the level of the crown (or ferrule) margin. A post essentially improves the ferrule effect that is provided by the partial fixed denture prosthesis. This paper also explores the difference between bio-mechanical failures of crowns caused by lack of retention or excess taper, versus failures due to a sub-optimal ferrule effect in crown and bridge prostheses.
Keyword
MeSH Terms
Figure
-
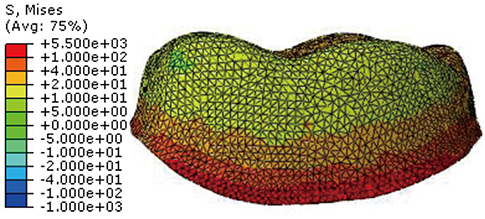
Fig. 1 Finite Element Analysis Diagram shows how a crown transmits most occlusal force (in red) to the level of the crown margin (photo courtesy of Dr. Seung-Ryong Ha, with permission from J Adv Prosthodont1).
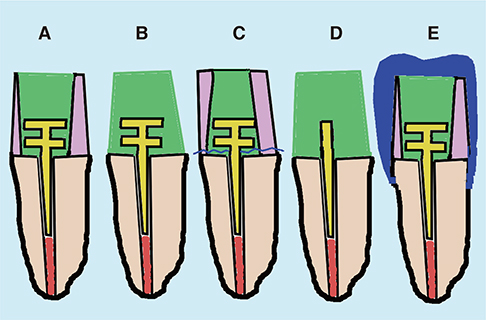
Fig. 2 Five examples of post/core restorations, where the core is retained only by the post, include situations where the abutment tooth structure has no undercuts to retain the core (A); the post is in a root tip (B); a tooth/core/post complex that fractured from the abutment was re-cemented and is retained only by a cement layer (C); a core separated from the post and was re-cemented and is retained only by the post cement (D); a core is not retained by tooth structure undercuts, but the crown margin is at 2.0 mm apical to the core on ferrule tooth structure (E). Only (E), and possibly (A), may be biomechanically stable.

Fig. 3 Finite Element Analysis Diagram of a post/core restoration shows how the post transmits moderate amounts of occlusal forces (in green) to the cemento-enamel-junction area of the post (where the crown or ferrule margin is often located), but also transmits most of the force (in red) to the root (photo courtesy of Dr. Prajna P. Shetty, with permission from Eur J Dent29).
Reference
-
1. Ha SR. Biomechanical three-dimensional finite element analysis of monolithic zirconia crown with different cement type. J Adv Prosthodont. 2015; 7:475–483.2. Pierrisnard L, Bohin F, Renault P, Barquins M. Coronoradicular reconstruction of pulpless teeth: a mechanical study using finite element analysis. J Prosthet Dent. 2002; 88:442–448.3. Mamoun JS. On the ferrule effect and the biomechanical stability of teeth restored with cores, posts, and crowns. Eur J Dent. 2014; 8:281–286.4. Zarone F, Sorrentino R, Apicella D, Valentino B, Ferrari M, Aversa R, Apicella A. Evaluation of the biomechanical behavior of maxillary central incisors restored by means of endocrowns compared to a natural tooth: a 3D static linear finite elements analysis. Dent Mater. 2006; 22:1035–1044.5. Sorrentino R, Aversa R, Ferro V, Auriemma T, Zarone F, Ferrari M, Apicella A. Three-dimensional finite element analysis of strain and stress distributions in endodontically treated maxillary central incisors restored with different post, core and crown materials. Dent Mater. 2007; 23:983–993.6. Ferrari M, Sorrentino R, Zarone F, Apicella D, Aversa R, Apicella A. Non-linear viscoelastic finite element analysis of the effect of the length of glass fiber posts on the biomechanical behaviour of directly restored incisors and surrounding alveolar bone. Dent Mater J. 2008; 27:485–498.7. Tjan AH, Whang SB. Resistance to root fracture of dowel channels with various thicknesses of buccal dentin walls. J Prosthet Dent. 1985; 53:496–500.8. Barkhordar RA, Radke R, Abbasi J. Effect of metal collars on resistance of endodontically treated teeth to root fracture. J Prosthet Dent. 1989; 61:676–678.9. Sorensen JA, Engelman MJ. Ferrule design and fracture resistance of endodontically treated teeth. J Prosthet Dent. 1990; 63:529–536.10. McLean A. Criteria for the predictably restorable endodontically treated tooth. J Can Dent Assoc. 1998; 64:652–656.11. Yang A, Lamichhane A, Xu C. Remaining coronal dentin and risk of fiber-reinforced composite post-core restoration failure: a meta-analysis. Int J Prosthodont. 2015; 28:258–264.12. Santos-Filho PC, Veríssimo C, Raposo LH, Noritomi MecEng PY, Marcondes Martins LR. Influence of ferrule, post system, and length on stress distribution of weakened root-filled teeth. J Endod. 2014; 40:1874–1878.13. Naumann M, Preuss A, Frankenberger R. Reinforcement effect of adhesively luted fiber reinforced composite versus titanium posts. Dent Mater. 2007; 23:138–144.14. Wu MK, van der Sluis LW, Wesselink PR. Comparison of mandibular premolars and canines with respect to their resistance to vertical root fracture. J Dent. 2004; 32:265–268.15. Plotino G, Grande NM, Falanga A, Di Giuseppe IL, Lamorgese V, Somma F. Dentine removal in the coronal portion of root canals following two preparation techniques. Int Endod J. 2007; 40:852–858.16. Zhu Z, Dong XY, He S, Pan X, Tang L. Effect of post placement on the restoration of endodontically treated teeth: A systematic review. Int J Prosthodont. 2015; 28:475–483.17. Assif D, Gorfil C. Biomechanical considerations in restoring endodontically treated teeth. J Prosthet Dent. 1994; 71:565–567.18. Martínez-Insua A, da Silva L, Rilo B, Santana U. Comparison of the fracture resistances of pulpless teeth restored with a cast post and core or carbon-fiber post with a composite core. J Prosthet Dent. 1998; 80:527–532.19. Plotino G, Grande NM, Bedini R, Pameijer CH, Somma F. Flexural properties of endodontic posts and human root dentin. Dent Mater. 2007; 23:1129–1135.20. Jørgensen KD. The relationship between retention and convergence angle in cemented veneer crowns. Acta Odontol Scand. 1955; 13:35–40.21. Shillingburg HT, Hobo S, Fisher DW. Preparations for cast gold restorations. 1st ed. Chicago: Quintessence Publishing Co.;1987.22. Kaufman EG, Coehlo DH, Colin L. Factors influencing the retention of cemented gold castings. J Prosthet Dent. 1961; 11:487–502.23. Parker MH, Calverley MJ, Gardner FM, Gunderson RB. New guidelines for preparation taper. J Prosthodont. 1993; 2:61–66.24. Ohm E, Silness J. The convergence angle in teeth prepared for artificial crowns. J Oral Rehabil. 1978; 5:371–375.25. Mack PJ. A theoretical and clinical investigation into the taper achieved on crown and inlay preparations. J Oral Rehabil. 1980; 7:255–265.26. Noonan JE Jr, Goldfogel MH. Convergence of the axial walls of full veneer crown preparations in a dental school environment. J Prosthet Dent. 1991; 66:706–708.27. Nordlander J, Weir D, Stoffer W, Ochi S. The taper of clinical preparations for fixed prosthodontics. J Prosthet Dent. 1988; 60:148–151.28. Singh SV, Bhat M, Gupta S, Sharma D, Satija H, Sharma S. Stress distribution of endodontically treated teeth with titanium alloy post and carbon fiber post with different alveolar bone height: A three-dimensional finite element analysis. Eur J Dent. 2015; 9:428–432.29. Shetty PP, Meshramkar R, Patil KN, Nadiger RK. A finite element analysis for a comparative evaluation of stress with two commonly used esthetic posts. Eur J Dent. 2013; 7:419–422.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Evaluation of the fracture resistance of all-ceramic zirconia posts by 3 different methods
- Effect of the shades of background substructures on the overall color of zirconia-based all-ceramic crowns
- Mechanical Properties of Quartz Fiber Post
- Color Comparison Of Various Post Systems With Empress 2 Crowns
- A clinical report of hybrid telescopic double crown denture with friction pin in a failed double crown denture case
