Subependymal Giant Cell Astrocytoma Presenting with Tumoral Bleeding: A Case Report
- Affiliations
-
- 1Department of Neurosurgery, Chonnam National University Medical School, Chonnam National University Hwasun Hospital, Hwasun, Korea. jung-ty@chonnam.ac.kr
- 2Department of Pathology, Chonnam National University Medical School, Chonnam National University Hwasun Hospital, Hwasun, Korea.
- 3Department of Radiology, Chonnam National University Medical School, Chonnam National University Hwasun Hospital, Hwasun, Korea.
- KMID: 2378304
- DOI: http://doi.org/10.14791/btrt.2017.5.1.37
Abstract
- We report a rare case of subependymal giant cell astrocytoma (SEGA) associated with tumoral bleeding in a pediatric patient without tuberous sclerosis complex (TSC). A 10-year-old girl presented with a 2-week history of an increasingly aggravating headache. Brain magnetic resonance imaging revealed an approximately 3.6-cm, well-defined, heterogeneously enhancing mass with multistage hemorrhages on the right-sided foramen of Monro. The tumor was completely resected using a transcallosal approach. Intraoperatively, the mass presented as a gray-colored firm tumor associated with acute and subacute hemorrhages. The origin of the mass was identified as the ventricular septum adjacent to the foramen of Monro. A pathological analysis revealed pleomorphic multinucleated eosinophilic tumor cells with abundant cytoplasm. These cells showed positive staining for the glial fibrillary acidic protein and S100 protein. A diagnosis of SEGA was established. The patient recovered without any neurological symptoms. There was no evidence of TSC. The radiological follow-up showed no recurrence for 2 years. This was a case of SEGA with intratumoral hemorrhage, for which a favorable outcome was achieved, without any neurological deficit after tumoral resection.
Keyword
MeSH Terms
Figure
-
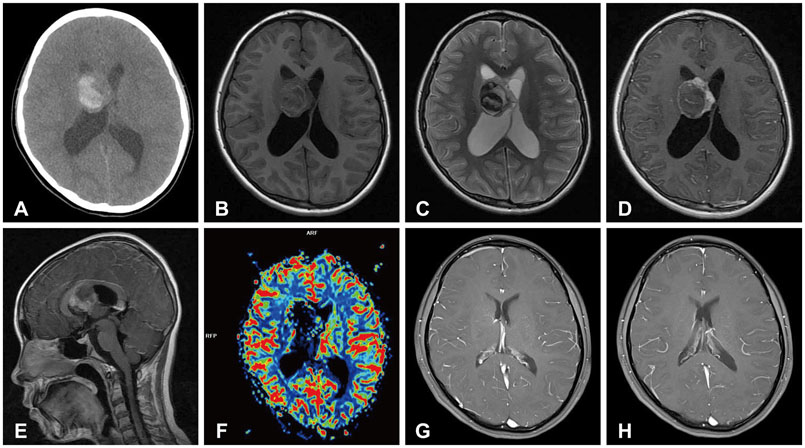
Fig. 1 Preoperative and postoperative radiological findings of subependymal giant cell astrocytoma with bleeding. A: A brain computed tomography scan showing acute hemorrhage on the right lateral ventricle. B: A brain magnetic resonance (MR) image showing an approximately 3.6-cm, well-defined mass in the right-sided foramen of Monro. The mass shows mixed low and high signal intensity on T1-weighted MR images. C: The mass shows mixed low and high signal intensity on T2-weighted MR images. D: Following gadolinium administration, the lesion demonstrates heterogeneous enhancement on axial images. E: The lesion is heterogeneously enhanced on peripheral solid area on sagittal images. F: Cerebral blood volume is focally increased on perfusion MR images. G and H: Recurrence is not observed for 2 years, based on T1-weighted enhanced MR images.

Fig. 2 Pathological findings of subependymal giant cell astrocytoma. A: Pathological analysis revealing tumor cells with many small vessels (hematoxylin and eosin staining, original magnification, ×40). B: The pleomorphic multinucleated eosinophilic tumor cells contain abundant cytoplasm (hematoxylin and eosin staining, original magnification, ×200). C: The tumor cells show focally positive staining for glial fibrillary acidic protein (original magnification, ×200). D: The tumor cells show positive staining for S100 protein (original magnification, ×200).
Reference
-
1. Adriaensen ME, Schaefer-Prokop CM, Stijnen T, Duyndam DA, Zonnenberg BA, Prokop M. Prevalence of subependymal giant cell tumors in patients with tuberous sclerosis and a review of the literature. Eur J Neurol. 2009; 16:691–696.
Article2. Beaumont TL, Godzik J, Dahiya S, Smyth MD. Subependymal giant cell astrocytoma in the absence of tuberous sclerosis complex: case report. J Neurosurg Pediatr. 2015; 16:134–137.
Article3. Stavrinou P, Spiliotopoulos A, Patsalas I, et al. Subependymal giant cell astrocytoma with intratumoral hemorrhage in the absence of tuberous sclerosis. J Clin Neurosci. 2008; 15:704–706.
Article4. Jung TY, Kim YH, Jung S, Baek HJ, Lee KH. The clinical characteristics of subependymal giant cell astrocytoma: five cases. Brain Tumor Res Treat. 2015; 3:44–47.
Article5. Kwiatkowska J, Wigowska-Sowinska J, Napierala D, Slomski R, Kwiatkowski DJ. Mosaicism in tuberous sclerosis as a potential cause of the failure of molecular diagnosis. N Engl J Med. 1999; 340:703–707.
Article6. Sterman H, Furlan AB, Matushita H, Teixeira MJ. Subependymal giant cell astrocytoma associated with tuberous sclerosis presenting with intratumoral bleeding. Case report and review of literature. Childs Nerv Syst. 2013; 29:335–339.
Article7. Ogiwara H, Morota N. Subependymal giant cell astrocytoma with intratumoral hemorrhage. J Neurosurg Pediatr. 2013; 11:469–472.
Article8. Northrup H, Krueger DA. International Tuberous Sclerosis Complex Consensus Group. Tuberous sclerosis complex diagnostic criteria update: recommendations of the 2012 International Tuberous Sclerosis Complex Consensus Conference. Pediatr Neurol. 2013; 49:243–254.9. Au KS, Williams AT, Gambello MJ, Northrup H. Molecular genetic basis of tuberous sclerosis complex: from bench to bedside. J Child Neurol. 2004; 19:699–709.
Article10. Dabora SL, Jozwiak S, Franz DN, et al. Mutational analysis in a cohort of 224 tuberous sclerosis patients indicates increased severity of TSC2, compared with TSC1, disease in multiple organs. Am J Hum Genet. 2001; 68:64–80.
Article11. Ichikawa T, Wakisaka A, Daido S, et al. A case of solitary subependymal giant cell astrocytoma: two somatic hits of TSC2 in the tumor, without evidence of somatic mosaicism. J Mol Diagn. 2005; 7:544–549.12. Wakai S, Yamakawa K, Manaka S, Takakura K. Spontaneous intracranial hemorrhage caused by brain tumor: its incidence and clinical significance. Neurosurgery. 1982; 10:437–444.13. Hamamoto O, Honorato DC, Brito HL, Souza-Queiróz L. [Intratumor hemorrhage in tuberous sclerosis. A case report]. Arq Neuropsiquiatr. 1994; 52:435–438.14. Sinson G, Sutton LN, Yachnis AT, Duhaime AC, Schut L. Subependymal giant cell astrocytomas in children. Pediatr Neurosurg. 1994; 20:233–239.
Article15. Beaumont TL, Limbrick DD, Smyth MD. Advances in the management of subependymal giant cell astrocytoma. Childs Nerv Syst. 2012; 28:963–968.
Article16. de Ribaupierre S, Dorfmüller G, Bulteau C, et al. Subependymal giant-cell astrocytomas in pediatric tuberous sclerosis disease: when should we operate? Neurosurgery. 2007; 60:83–89. discussion 89-90.17. Fujiwara S, Takaki T, Hikita T, Nishio S. Subependymal giant-cell astrocytoma associated with tuberous sclerosis. Do subependymal nodules grow? Childs Nerv Syst. 1989; 5:43–44.18. Waga S, Yamamoto Y, Kojima T, Sakakura M. Massive hemorrhage in tumor of tuberous sclerosis. Surg Neurol. 1977; 8:99–101.19. Barbosa-Coutinho LM, Lima EL, Gadret RO, Ferreira NP. [Massive intratumor hemorrhage in tuberous sclerosis. Autopsy study of a case]. Arq Neuropsiquiatr. 1991; 49:465–470.20. Kalina P, Drehobl KE, Greenberg RW, Black KS, Hyman RA. Hemorrhagic subependymal giant cell astrocytoma. Pediatr Radiol. 1995; 25:66–67.
Article21. Kim SK, Wang KC, Cho BK, et al. Biological behavior and tumorigenesis of subependymal giant cell astrocytomas. J Neurooncol. 2001; 52:217–225.22. Henderson MA, Fakiris AJ, Timmerman RD, Worth RM, Lo SS, Witt TC. Gamma knife stereotactic radiosurgery for low-grade astrocytomas. Stereotact Funct Neurosurg. 2009; 87:161–167.
Article23. Park YG, Kim EY, Chang JW, Chung SS. Volume changes following gamma knife radiosurgery of intracranial tumors. Surg Neurol. 1997; 48:488–493.
Article24. Wang LW, Shiau CY, Chung WY, et al. Gamma knife surgery for low-grade astrocytomas: evaluation of long-term outcome based on a 10-year experience. J Neurosurg. 2006; 105 Suppl:127–132.
Article25. Park KJ, Kano H, Kondziolka D, Niranjan A, Flickinger JC, Lunsford LD. Gamma knife surgery for subependymal giant cell astrocytomas. Clinical article. J Neurosurg. 2011; 114:808–813.26. Krueger DA, Care MM, Holland K, et al. Everolimus for subependymal giant-cell astrocytomas in tuberous sclerosis. N Engl J Med. 2010; 363:1801–1811.
Article27. Franz DN, Belousova E, Sparagana S, et al. Efficacy and safety of everolimus for subependymal giant cell astrocytomas associated with tuberous sclerosis complex (EXIST-1): a multicentre, randomised, placebo-controlled phase 3 trial. Lancet. 2013; 381:125–132.
Article28. Franz DN, Leonard J, Tudor C, et al. Rapamycin causes regression of astrocytomas in tuberous sclerosis complex. Ann Neurol. 2006; 59:490–498.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A case of tuberous sclerosis developing with subependymal giant-cell astrocytoma
- A Case of Subependymal Giant Cell Astrocytoma in the Absence of Tuberous Sclerosis: Case Report
- A Case of Tuberous Sclerosis Complex Developing with Subependymal Giant-Cell Astrocytoma and Hydrocephalus
- Subependymal Giant Cell Astrocytoma with a Large Third Ventricular Hematoma
- A Case of Subependymal Giant Cell Astrocytoma associated with Tuberous Sclerosis(Case Report)
