Missed Cauda Equina Syndrome after Burst Fracture of the Lumbar Spine
- Affiliations
-
- 1Department of Neurosurgery, Dongguk University College of Medicine, Seoul, Korea.
- 2Department of Neurosurgery, Dongguk University Ilsan Hospital, Dongguk University College of Medicine, Goyang, Korea. ktcho21@naver.com
- KMID: 2378282
- DOI: http://doi.org/10.13004/kjnt.2015.11.2.175
Abstract
- Cauda equina syndrome (CES) is often defined as a complex of symptoms and signs consisting of low back pain, bilateral sciatica, lower extremity weakness, saddle anesthesia, and bowel and bladder dysfunction. CES is considered to be neurosurgical emergency. Delayed or missed diagnosis of CES can result in serious morbidity and neurological sequelae. However, the diagnosis of CES is often difficult when one or more of these symptoms are absent or when these symptoms develop asymmetrically or incompletely. We report a case of urinary retention and sphincter dysfunction without sciatica or motor weakness following an L3 burst fracture in a 52-year-old male and discuss the atypical presentation of CES and treatment of traumatic CES.
Keyword
MeSH Terms
Figure
-
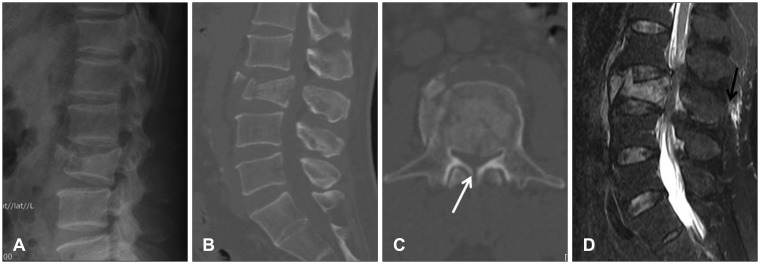
FIGURE 1 Lumbar spine images immediately after trauma. Plain lateral radiography (A) and sagittal (B) view of the computed tomography scan show the L3 burst fracture and about 50% height loss in the vertebral body. Midsagittal spinal canal diameter estimated at the level of the fracture in the transpedicular axial cut is 7.92 mm, which represents 55% of narrowing of the spinal canal compared to the normal level. Spinous process fracture is also seen (white arrow) (C). Fat-suppressed T2-weighted magnetic resonance imaging reveals suspicious supraspinous ligament injury (black arrow) (D).
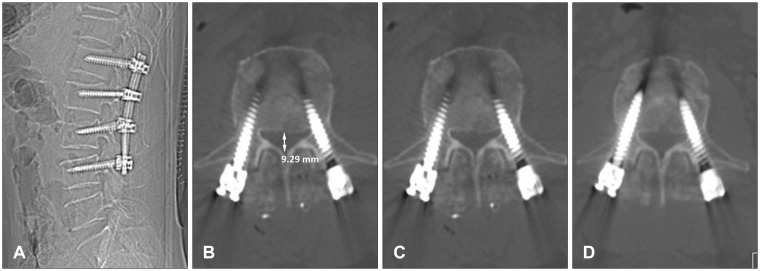
FIGURE 2 Postoperative lumbar spine images. Plain lateral radiography (A) and sagittal (B) view of the computed tomography scan show restoration of spinal alignment and slight reduction of the retropulsed bony fragment. Midsagittal spinal canal diameter is 9.29 mm, which was slightly increased compared to the preoperative images (C). Midsagittal spinal canal diameter is 10.94 mm 3 months after the surgery (D).
Reference
-
1. Balasubramanian K, Kalsi P, Greenough CG, Kuskoor Seetharam MP. Reliability of clinical assessment in diagnosing cauda equina syndrome. Br J Neurosurg. 2010; 24:383–386. PMID: 20726746.
Article2. Bell DA, Collie D, Statham PF. Cauda equina syndrome: what is the correlation between clinical assessment and MRI scanning? Br J Neurosurg. 2007; 21:201–203. PMID: 17453789.3. Bradford DS, McBride GG. Surgical management of thoracolumbar spine fractures with incomplete neurologic deficits. Clin Orthop Relat Res. 1987; (218):201–216. PMID: 3568482.
Article4. Caputo LA, Cusimano MD. Atypical presentation of cauda equina syndrome. J Can Chiropr Assoc. 2002; 46:31–38.5. Celik EC, Kabatas S, Karatas M. Atypical presentation of cauda equina syndrome secondary to lumbar disc herniation. J Back Musculoskelet Rehabil. 2012; 25:1–3. PMID: 22398260.
Article6. Dai LY, Wang XY, Jiang LS. Neurologic recovery from thoracolumbar burst fractures: is it predicted by the amount of initial canal encroachment and kyphotic deformity? Surg Neurol. 2007; 67:232–237. discussion 238PMID: 17320624.
Article7. Domen PM, Hofman PA, van Santbrink H, Weber WE. Predictive value of clinical characteristics in patients with suspected cauda equina syndrome. Eur J Neurol. 2009; 16:416–419. PMID: 19490073.
Article8. Fairbank J, Hashimoto R, Dailey A, Patel AA, Dettori JR. Does patient history and physical examination predict MRI proven cauda equina syndrome? Evid Based Spine Care J. 2011; 2:27–33. PMID: 23230403.
Article9. Fraser S, Roberts L, Murphy E. Cauda equina syndrome: a literature review of its definition and clinical presentation. Arch Phys Med Rehabil. 2009; 90:1964–1968. PMID: 19887225.
Article10. Gitelman A, Hishmeh S, Morelli BN, Joseph SA Jr, Casden A, Kuflik P, et al. Cauda equina syndrome: a comprehensive review. Am J Orthop (Belle Mead NJ). 2008; 37:556–562. PMID: 19104682.11. Gooding BW, Higgins MA, Calthorpe DA. Does rectal examination have any value in the clinical diagnosis of cauda equina syndrome? Br J Neurosurg. 2013; 27:156–159. PMID: 23113877.
Article12. Harrop JS, Hunt GE Jr, Vaccaro AR. Conus medullaris and cauda equina syndrome as a result of traumatic injuries: management principles. Neurosurg Focus. 2004; 16:e4. PMID: 15202874.
Article13. Herndon WA, Galloway D. Neurologic return versus cross-sectional canal area in incomplete thoracolumbar spinal cord injuries. J Trauma. 1988; 28:680–683. PMID: 3367414.14. Hu SS, Capen DA, Rimoldi RL, Zigler JE. The effect of surgical decompression on neurologic outcome after lumbar fractures. Clin Orthop Relat Res. 1993; (288):166–173. PMID: 8458130.
Article15. Kaneda K, Taneichi H, Abumi K, Hashimoto T, Satoh S, Fujiya M. Anterior decompression and stabilization with the Kaneda device for thoracolumbar burst fractures associated with neurological deficits. J Bone Joint Surg Am. 1997; 79:69–83. PMID: 9010188.16. Kim NH, Lee HM, Chun IM. Neurologic injury and recovery in patients with burst fracture of the thoracolumbar spine. Spine (Phila Pa 1976). 1999; 24:290–293. discussion 294PMID: 10025025.
Article17. Kim TW, Yoon JW, Heo W, Park HS, Rhee DY. Lumbar Disc Herniation Presenting Cauda Equina Syndrome. J Korean Neurosurg Soc. 2006; 39:40–45.18. Kingwell SP, Curt A, Dvorak MF. Factors affecting neurological outcome in traumatic conus medullaris and cauda equina injuries. Neurosurg Focus. 2008; 25:E7. PMID: 18980481.
Article19. Kostuik JP, Harrington I, Alexander D, Rand W, Evans D. Cauda equina syndrome and lumbar disc herniation. J Bone Joint Surg Am. 1986; 68:386–391. PMID: 2936744.
Article20. Meves R, Avanzi O. Correlation between neurological deficit and spinal canal compromise in 198 patients with thoracolumbar and lumbar fractures. Spine (Phila Pa 1976). 2005; 30:787–791. PMID: 15803082.
Article21. Mohanty SP, Venkatram N. Does neurological recovery in thoracolumbar and lumbar burst fractures depend on the extent of canal compromise? Spinal Cord. 2002; 40:295–299. PMID: 12037711.
Article22. O'Laoire SA, Crockard HA, Thomas DG. Prognosis for sphincter recovery after operation for cauda equina compression owing to lumbar disc prolapse. Br Med J (Clin Res Ed). 1981; 282:1852–1854.23. Orendácová J, Cízková D, Kafka J, Lukácová N, Marsala M, Sulla I, et al. Cauda equina syndrome. Prog Neurobiol. 2001; 64:613–637. PMID: 11311464.24. Sylvester PA, McLoughlin J, Sibley GN, Dorman PJ, Kabala J, Ormerod IE. Neuropathic urinary retention in the absence of neurological signs. Postgrad Med J. 1995; 71:747–748. PMID: 8552542.
Article25. Thongtrangan I, Le H, Park J, Kim DH. Cauda equina syndrome in patients with low lumbar fractures. Neurosurg Focus. 2004; 16:e6. PMID: 15202876.26. Wang US, Ju CI, Kim SW, Wang HS, Lee SM. Short Segment Screw Fixation without Fusion for Low Lumbar Burst Fracture: Severe Canal Compromise but Neurologically Intact Cases. Korean J Neurotrauma. 2013; 9:101–105.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Predictable Imaging Signs of Cauda Equina Entrapment in Thoracolumbar and Lumbar Burst Fractures with Greenstick Lamina Fractures
- Bisected Vertebral Body Fracture Trapping Cauda Equina: A Case Report
- Posterior Epidural Migration of a Sequestrated Intervertebral lumbar Disc with Cauda Equina Syndrome: Two Cases Report
- Cauda Equina Syndrome Occurred by Adhesive Arachnoiditis of the Lumbar Spine with an Unknown Cause
- Thoracic Spine Tumor Mimicking Cauda Equina Syndrome
