Intramuscular hemangiomas on the masseter muscle and orbicularis oris muscle: a report of two cases
- Affiliations
-
- 1Department of Oral and Maxillofacial Surgery, Inha University College of Medicine, Incheon, Korea. kik@inha.ac.kr
- 2Department of Pathology, Inha University School of Medicine, Incheon, Korea.
- KMID: 2377017
- DOI: http://doi.org/10.5125/jkaoms.2017.43.2.125
Abstract
- Intramuscular hemangioma (IMH) is a rare vascular disease involving skeletal muscle, comprising only 0.8% of hemangiomas. About 10% to 15% of IMHs occur in the head and neck region, mostly involving the masseter muscle. IMH occurs mostly in childhood, but is often not found until unexpected enlargement, pain, or cosmetic asymmetry occurs in adulthood. Several non-surgical treatments including cryotherapy, sclerosant injection, and arterial ligature have been described, but complete surgical resection is the curative intervention. In this report, we present two rare cases of IMH. One IMH case in a 48-year-old male occurred in the masseter muscle feeding from the transverse facial artery. Embolization of the distal branch of the facial artery was first conducted, and then the buccal mass was removed surgically via the intraoral approach. A second IMH case in a 58-year-old female occurred in the orbicularis oris muscle feeding from the superior labial artery, and the mass was excised surgically without embolization.
MeSH Terms
Figure
-

Fig. 1 Case 1. Preoperative clinical view. Swelling of the patient's left cheek is shown (arrow). A. Facial view. B. Lateral view.
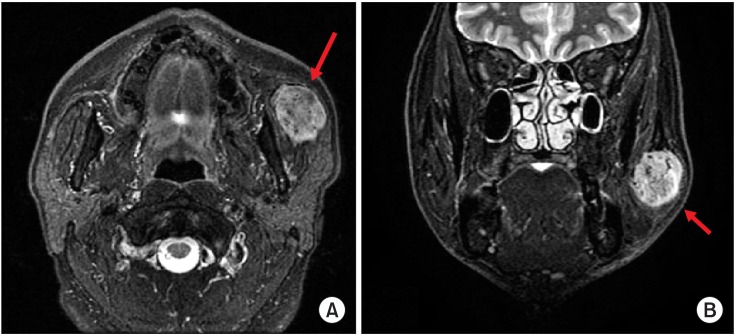
Fig. 2 Case 1. Preoperative magnetic resonance imaging. A well-marginated mass (arrows) was found in the left masseter muscle. A. Axial view. B. Coronal view.
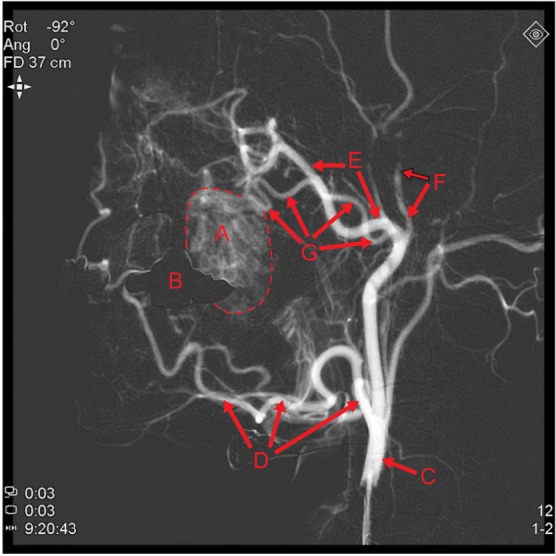
Fig. 3 Case 1. Preoperative external carotid angiography, lateral view. The main mass (‘A’) is shown near the overlapped image of a dental prosthesis (‘B’). It is feeding from the transverse facial artery (‘G’) and maxillary artery (‘E’). (‘A’: main mass, ‘B’: overlapped image of dental prosthesis [maxillary left implant and maxillary right 3-unit bridge], ‘C’: external carotid artery, ‘D’: facial artery, ‘E’: maxillary artery, ‘F’: superficial temporal artery, ‘G’: transverse facial artery [main])

Fig. 4 Case 1. Preoperative external carotid angiography, lateral view. The mass (‘A’) became blushed by contrast agent injection (A-C), then gradually disappeared with time (D). (‘A’: main mass, ‘B’: overlapped image of dental prosthesis [maxillary left implant and maxillary right 3-unit bridge])

Fig. 5 Case 1. Procedure of embolization. (A) Selection of the distal branch of the transverse facial artery was achieved by Prowler select plus. (B) After embolization by polyvinyl alcohol particle injection (no picture), the contrast agent was injected locally to the selected site, and back pressure was observed intensively at the backside of the selected site. (C) Contrast agent was injected into the external carotid angiography again, and the mass was faintly visualized although sufficient time had passed. (‘A’: main mass, ‘B’: overlapped image of dental prosthesis [maxillary left implant and maxillary right 3-unit bridge])
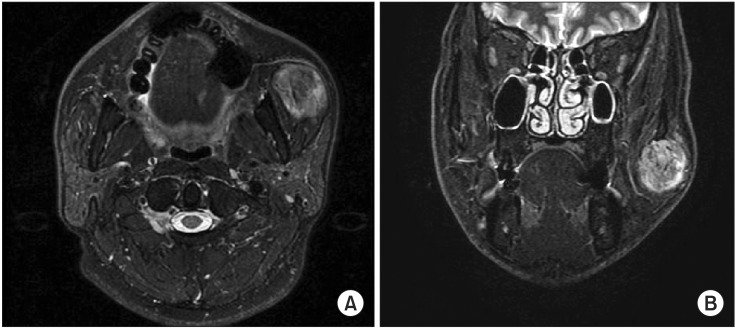
Fig. 6 Case 1. Post-embolization magnetic resonance imaging. No significant changes appeared. A. Axial view. B. Coronal view.

Fig. 7 Case 1. The main mass of the patient.

Fig. 8 Case 1. Microscopic view of the mass. A. Developed vessels with proliferation of endothelial cells between skeletal muscle tissue can be identified (H&E staining, ×100). B. Capillaries are predominant, and large vessels are seen occasionally (H&E staining, ×200). Many adipose tissues can be observed (C: H&E staining, ×40), and large vessels (possibly from feeding vessels) are also observed within the mass (D: H&E staining, ×40).

Fig. 9 Case 2. Preoperative clinical view of the patient. The patient's upper lip is shown with swelling in the right angular region.

Fig. 10 Case 2. Preoperative magnetic resonance imaging (MRI). A well-marginated mass was found in the right upper lip on MRI STIR (short-T1 inversion recovery) axial images (A) and T2 coronal images (B).
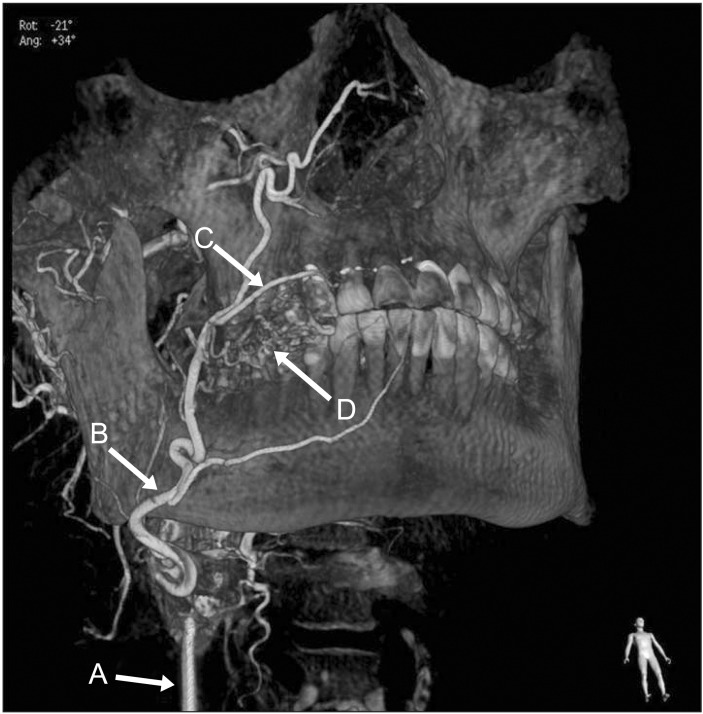
Fig. 11 Case 2. Preoperative angiography of the patient. The mass was feeding from small branches of the superior labial artery. (‘A’: external carotid artery, ‘B’: facial artery, ‘C’: superior labial artery, ‘D’: main mass)
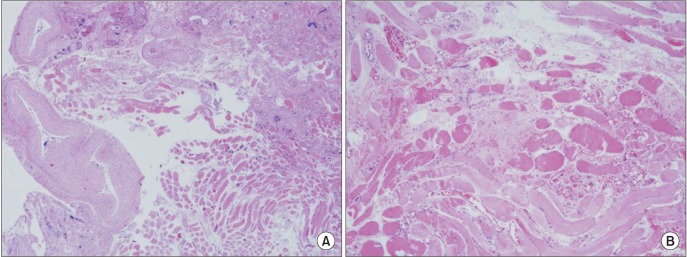
Fig. 12 Case 2. Microscopic view of the mass of the patient. Large vessels (may be from feeding vessels) are observed in the lateral side of the mass (A: H&E staining, ×40), and developed vessels with proliferation of endothelial cells between skeletal muscle tissues can be identified (B: H&E staining, ×100).

Fig. 13 Case 2. Immunohistochemical view of the mass. The endothelial cells are positive for CD34 (×100).
Reference
-
1. Watson WL, McCarthy WD. Blood and lymph vessel tumors. Srug Gynecol Obstet. 1940; 71:569–588.2. Wolf GT, Daniel F, Krause CJ, Kaufman RS. Intramuscular hemangioma of the head and neck. Laryngoscope. 1985; 95:210–213. PMID: 3968956.
Article3. Gordon JS, Mandel L. Masseteric intramuscular hemangioma: case report. J Oral Maxillofac Surg. 2014; 72:2192–2196. PMID: 24976110.
Article4. Odabasi AO, Metin KK, Mutlu C, Başak S, Erpek G. Intramuscular hemangioma of the masseter muscle. Eur Arch Otorhinolaryngol. 1999; 256:366–369. PMID: 10473832.
Article5. Chan MJ, McLean NR, Soames JV. Intramuscular haemangioma of the orbicularis oris muscle. Br J Oral Maxillofac Surg. 1992; 30:192–194. PMID: 1622968.
Article6. Kinni ME, Webb RI, Christensen RE. Intramuscular hemangioma of the orbicularis oris muscle: report of case. J Oral Surg. 1981; 39:780–782. PMID: 6944460.7. Righini CA, Berta E, Atallah I. Intramuscular cavernous hemangioma arising from the masseter muscle. Eur Ann Otorhinolaryngol Head Neck Dis. 2014; 131:57–59. PMID: 23845293.
Article8. Ichimura K, Nibu K, Tanaka T. Essentials of surgical treatment for intramasseteric hemangioma. Eur Arch Otorhinolaryngol. 1995; 252:125–129. PMID: 7662343.
Article9. Righi S, Boffano P, Malvè L, Rossi P, Zanardi F, Pateras D. Intramural perimasseteric hemangiomas of the inner cheek. J Craniofac Surg. 2015; 26:959–960. PMID: 25974807.
Article10. Chaudry MI, Manzoor MU, Turner RD, Turk AS. Diagnostic imaging of vascular anomalies. Facial Plast Surg. 2012; 28:563–574. PMID: 23188683.
Article11. Donnelly LF, Adams DM, Bisset GS 3rd. Vascular malformations and hemangiomas: a practical approach in a multidisciplinary clinic. AJR Am J Roentgenol. 2000; 174:597–608. PMID: 10701595.12. Flors L, Leiva-Salinas C, Maged IM, Norton PT, Matsumoto AH, Angle JF, et al. MR imaging of soft-tissue vascular malformations: diagnosis, classification, and therapy follow-up. Radiographics. 2011; 31:1321–1340. PMID: 21918047.
Article13. Yilmaz S, Kozakewich HP, Alomari AI, Fishman SJ, Mulliken JB, Chaudry G. Intramuscular capillary-type hemangioma: radiologic-pathologic correlation. Pediatr Radiol. 2014; 44:558–565. PMID: 24487677.
Article14. Rosbe KW, Hess CP, Dowd CF, Frieden IJ. Masseteric venous malformations: diagnosis, treatment, and outcomes. Otolaryngol Head Neck Surg. 2010; 143:779–783. PMID: 21109077.
Article15. Lee SK, Kwon SY. Intramuscular cavernous hemangioma arising from masseter muscle: a diagnostic dilemma (2006: 12b). Eur Radiol. 2007; 17:854–857. PMID: 17225132.
Article16. Allen PW, Enzinger FM. Hemangioma of skeletal muscle. An analysis of 89 cases. Cancer. 1972; 29:8–22. PMID: 5061701.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Cavernous Hemangioma of the Masseter Muscle
- Intramuscular hemangioma formation in the masseter muscle: a case report
- Intramuscular Hemangioma of the Sternocleidomastoid Muscle: An Unusual Neck Mass
- A hemangioma in the masseter muscle: a case report
- The effects of facial denervation on facial muscles and bones in growing rabbits
