A Case of Cap Polyposis with Epidermal Nevus in an Infant
- Affiliations
-
- 1Department of Pediatrics, Chonbuk National University Medical School, Chonbuk National University Hospital, Jeonju, Korea. hwaph@jbnu.ac.kr
- 2Research Institute of Clinical Medicine-Biomedical Research Institute, Chonbuk National University Hospital, Jeonju, Korea.
- 3Department of Pathology, Chonbuk National University Medical School, Chonbuk National University Hospital, Jeonju, Korea.
- 4Division of Pediatric Surgery, Chonbuk National University Medical School, Chonbuk National University Hospital, Jeonju, Korea.
- KMID: 2375092
- DOI: http://doi.org/10.3346/jkms.2017.32.5.880
Abstract
- Cap polyposis is extremely rare in children. We report a case of an 11-month-old male infant who visited our hospital because of rectal prolapse and small amount of hematochezia lasting several days. He also had an epidermal nevus in the sacral area. Colonoscopy showed erythematous, multilobulated, circumferential, polypoid lesions with mucoid discharge from the rectum. He was diagnosed with cap polyposis by endoscopy and histologic examination. He was treated with surgical resection, and was closely followed up. In the relevant literature, there is no report of cap polyposis in an infant. We report the first case of cap polyposis in the youngest infant.
Keyword
MeSH Terms
Figure
-

Fig. 1 This picture shows asymmetric, bright, brown colored, diffuse groups of verrucous plaque, and an elevated macular epidermal nevus located in the lower back and sacral area.
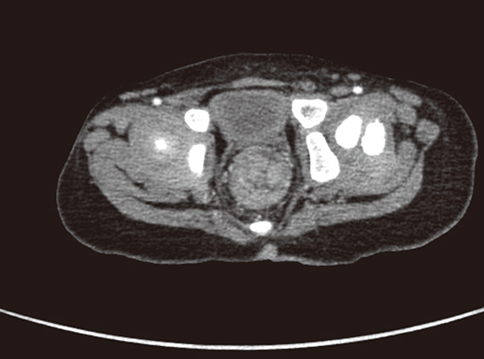
Fig. 2 CT image shows well-enhanced, multiple polypoid lesions about 1 cm in size located at 5 cm above the anal verge. Multiple lymph node enlargement was noted. CT = computed tomography.

Fig. 3 Barium enema study shows multilobulated mass-like mucosal lesions in the recto-anal area. There was no evidence of mucosal destruction or obstruction from the rectum to the ascending colon.
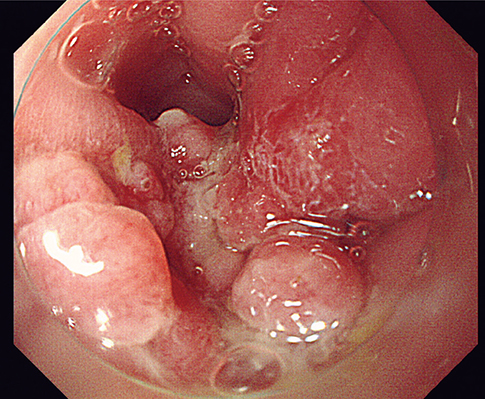
Fig. 4 Multilobulated, 4–6 cm in size polypoid groups were seen from the anus to the proximal rectum on colonoscopic view.
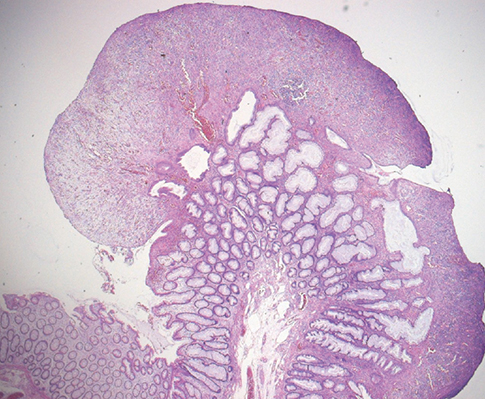
Fig. 5 Hyperplastic crypts covered with calcified granulation tissue were revealed on histologic examination (H & E, ×100). H & E = hematoxylin and eosin.
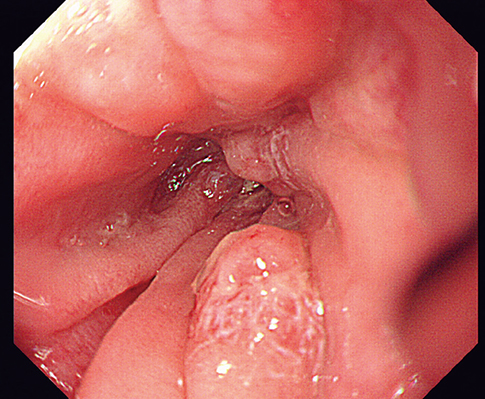
Fig. 6 About 1-cm in size small remnant mucosal polypoid lesions were seen at the inner anus on follow-up endoscopy.
Reference
-
1. Williams GT, Bussey HJ, Morson BC. Inflammatory “cap” polyps of the large intestine. Br J Surg. 1985; 72:S133.2. Mason M, Faizi SA, Fischer E, Rajput A. Inflammatory cap polyposis in a 42-year-old male. Int J Surg Case Rep. 2013; 4:351–353.3. Li JH, Leong MY, Phua KB, Low Y, Kader A, Logarajah V, Ong LY, Chua JH, Ong C. Cap polyposis: a rare cause of rectal bleeding in children. World J Gastroenterol. 2013; 19:4185–4191.4. Papaconstantinou I, Karakatsanis A, Benia X, Polymeneas G, Kostopoulou E. Solitary rectal cap polyp: case report and review of the literature. World J Gastrointest Surg. 2012; 4:157–162.5. Mall V, Heinen F, Uhl M, Wellens E, Korinthenberg R. CNS lipoma in patients with epidermal nevus syndrome. Neuropediatrics. 2000; 31:175–179.6. Géhénot M, Colombel JF, Wolschies E, Quandalle P, Gower P, Lecomte-Houcke M, Van Kruiningen H, Cortot A. Cap polyposis occurring in the postoperative course of pelvic surgery. Gut. 1994; 35:1670–1672.7. Suzuki H, Sato M, Akutsu D, Sugiyama H, Sato T, Mizokami Y. A case of cap polyposis remission by betamethasone enema after antibiotics therapy including Helicobacter pylori eradication. J Gastrointestin Liver Dis. 2014; 23:203–206.8. Oiya H, Okawa K, Aoki T, Nebiki H, Inoue T. Cap polyposis cured by Helicobacter pylori eradication therapy. J Gastroenterol. 2002; 37:463–466.9. Akamatsu T, Nakamura N, Kawamura Y, Shinji A, Tateiwa N, Ochi Y, Katsuyama T, Kiyosawa K. Possible relationship between Helicobacter pylori infection and cap polyposis of the colon. Helicobacter. 2004; 9:651–656.10. Abid S, Khawaja A, Bhimani SA, Ahmad Z, Hamid S, Jafri W. The clinical, endoscopic and histological spectrum of the solitary rectal ulcer syndrome: a single-center experience of 116 cases. BMC Gastroenterol. 2012; 12:72.11. Singh B, Mortensen NJ, Warren BF. Histopathological mimicry in mucosal prolapse. Histopathology. 2007; 50:97–102.12. Oriuchi T, Kinouchi Y, Kimura M, Hiwatashi N, Hayakawa T, Watanabe H, Yamada S, Nishihira T, Ohtsuki S, Toyota T. Successful treatment of cap polyposis by avoidance of intraluminal trauma: clues to pathogenesis. Am J Gastroenterol. 2000; 95:2095–2098.13. Ng KH, Mathur P, Kumarasinghe MP, Eu KW, Seow-Choen F. Cap polyposis: further experience and review. Dis Colon Rectum. 2004; 47:1208–1215.14. Bookman ID, Redston MS, Greenberg GR. Successful treatment of cap polyposis with infliximab. Gastroenterology. 2004; 126:1868–1871.15. Maunoury V, Breisse M, Desreumaux P, Gambiez L, Colombel JF. Infliximab failure in cap polyposis. Gut. 2005; 54:313–314.16. Isomoto H, Urata M, Nakagoe T, Sawai T, Nomoto T, Oda H, Nomura N, Takeshima F, Mizuta Y, Murase K, et al. Proximal extension of cap polyposis confirmed by colonoscopy. Gastrointest Endosc. 2001; 54:388–391.17. Farajzadeh S, Zahedi MJ, Moghaddam SD. A new gastrointestinal finding in Proteus syndrome: report of a case of multiple colonic hemangiomas. Int J Dermatol. 2006; 45:135–138.18. Romiti R, Arnone M, Sotto MN. Epidermal naevus with Darier’s disease-like changes in a patient with Gardner’s syndrome. J Am Acad Dermatol. 2000; 43:380–382.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Acantholytic Dyskeratotic Epidermal Nevus
- A Case of Congenital Melanocytic Nevus Combined with an Epidermal Cyst
- Remission of Cap Polyposis Maintained for More Than Three Years after Infliximab Treatment
- A Case of Diffuse Epidermal Nevi in the Neonate
- A Case of Cap Polyposis Complicated with Idiopathic Retroperitoneal Fibrosis
