Korean J Gastroenterol.
2011 Nov;58(5):275-279. 10.4166/kjg.2011.58.5.275.
A Case of Cap Polyposis Complicated with Idiopathic Retroperitoneal Fibrosis
- Affiliations
-
- 1Department of Internal Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. jinyong33.kim@samsung.com
- KMID: 1026370
- DOI: http://doi.org/10.4166/kjg.2011.58.5.275
Abstract
- An optimal treatment for cap polyposis has not been established. Several treatment approaches, including anti-inflammatory agents, antibiotics, immunomodulators, and endoscopic therapy have been described. Surgical resection of the affected colon and rectum may be indicated for patients with persistent disease. Repeat surgery is indicated in cases of recurrence after surgery. However, symptomatic polyposis may still recur, and spontaneous resolution of cap polyposis is possible. We report a case of recurrent cap polyposis complicated with retroperitoneal fibrosis after inadequate low anterior resection with a positive resection margin. Surgical approaches for the treatment of cap polyposis should be carefully considered before treatment.
MeSH Terms
Figure
-
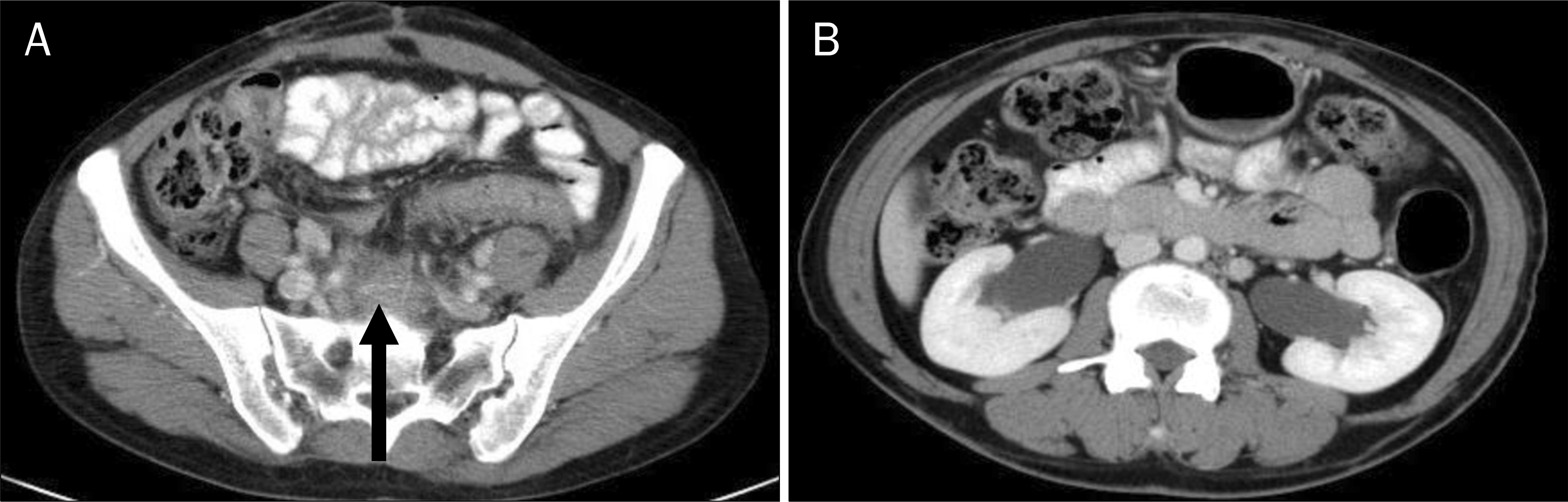
Fig. 1. Abdominopelvic CT finding. (A) It showed soft tissue infiltrations (arrow) surrounding the presacral space. (B) Associated hydronephroureterosis was noted.
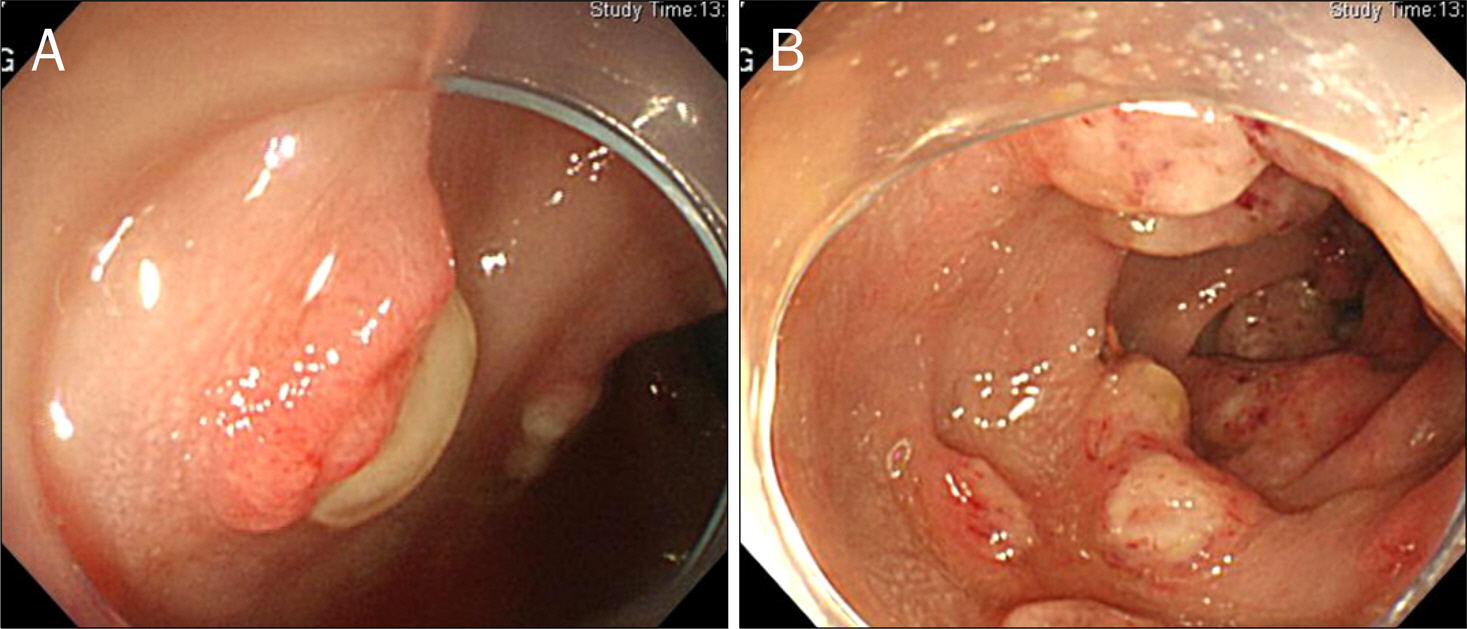
Fig. 2. Colonoscopic image. Sessile polyps with caps of purulent exudates were observed.
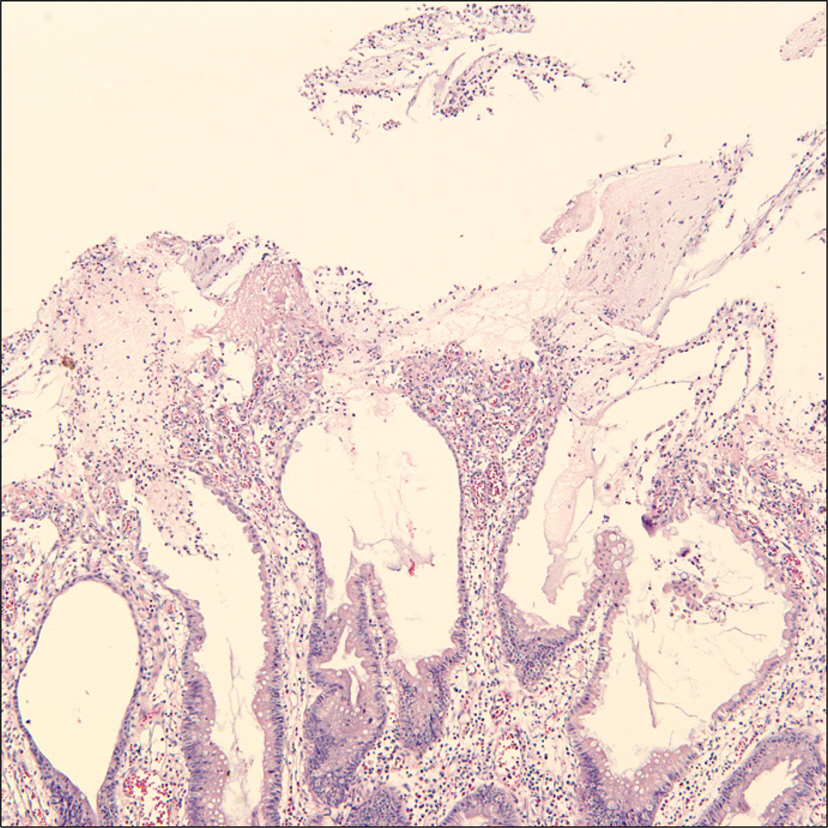
Fig. 3. Pathologic finding of colonoscopic biopy. It showed the surface of polyps covered by exudates (H&E, ×100).
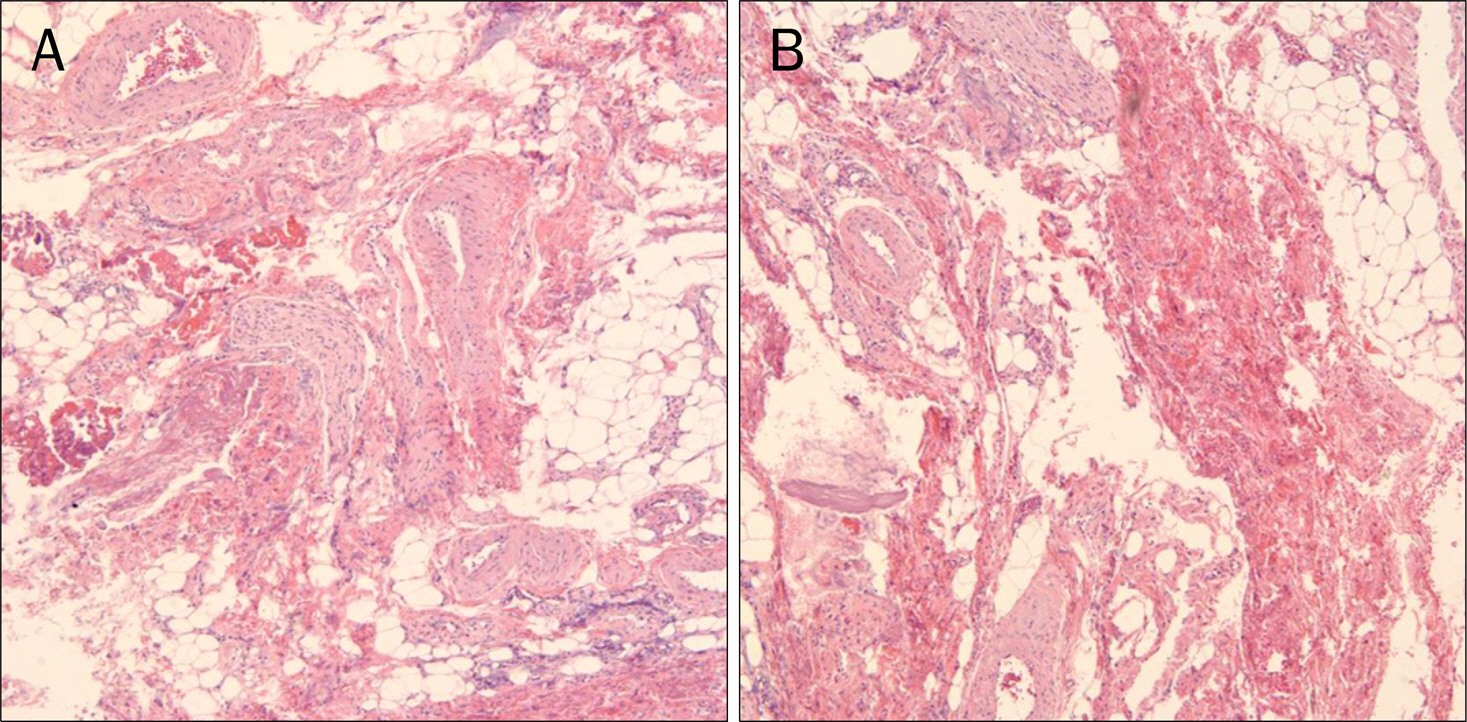
Fig. 4. Pathologic findings of retroperitoneal biopsy. (A) It showed fibroblast and lymphocyte infiltration in fibrosis (H&E, ×100). (B) Numerous blood vessels and peripheral nerves were observed due to secondary post- inflammatory change (H&E, ×100).
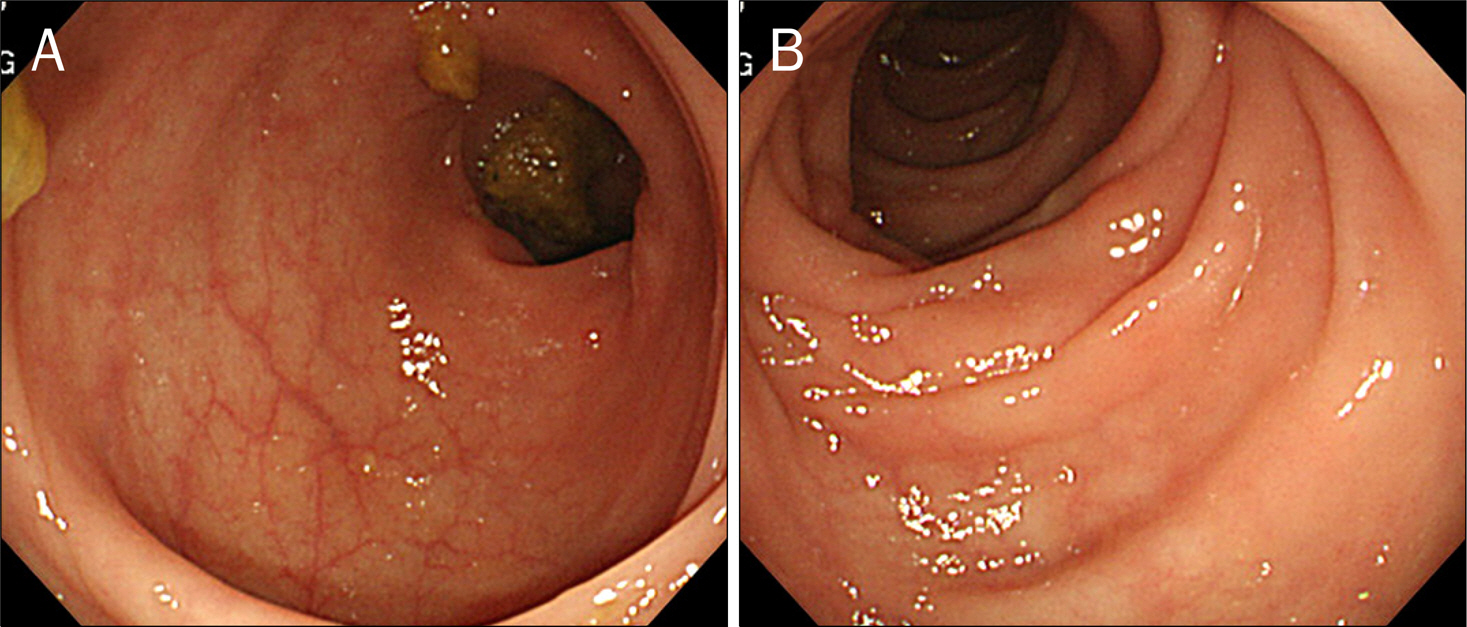
Fig. 5. Follow-up endoscopic images. It showed resolved cap polyposis.
Reference
-
References
1. Esaki M, Matsumoto T, Kobayashi H, et al. Cap polyposis of the colon and rectum: an analysis of endoscopic findings. Endoscopy. 2001; 33:262–266.
Article2. Géhénot M, Colombel JF, Wolschies E, et al. Cap polyposis occurring in the postoperative course of pelvic surgery. Gut. 1994; 35:1670–1672.
Article3. Campbell AP, Cobb CA, Chapman RW, et al. Cap polyposis–an unusual cause of diarrhoea. Gut. 1993; 34:562–564.
Article4. Ohkawara T, Kato M, Nakagawa S, et al. Spontaneous resolution of cap polyposis: case report. Gastrointest Endosc. 2003; 57:599–602.
Article5. Gilkeson GS, Allen NB. Retroperitoneal fibrosis. A true connective tissue disease. Rheum Dis Clin North Am. 1996; 22:23–38.6. Vaglio A, Salvarani C, Buzio C. Retroperitoneal fibrosis. Lancet. 2006; 367:241–251.
Article7. Hautekeete ML, Babany G, Marcellin P, et al. Retroperitoneal fibrosis after surgery for aortic aneurysm in a patient with periarter-itis nodosa: successful treatment with corticosteroids. J Intern Med. 1990; 228:533–536.
Article8. Wilson MC, Berry AR, McNair TJ, Thomson JW. Obstructive urop-athy after pan-proctocolectomy for ulcerative colitis. Gut. 1980; 21:808–809.
Article9. Williams GT, Bussey HJ, Morson BC. Inflammatory ‘cap’ polyps of the large intestine. Br J Surg. 1985; 72:S133.10. Oriuchi T, Kinouchi Y, Kimura M, et al. Successful treatment of cap polyposis by avoidance of intraluminal trauma: clues to pathogenesis. Am J Gastroenterol. 2000; 95:2095–2098.
Article11. Akamatsu T, Nakamura N, Kawamura Y, et al. Possible relationship between Helicobacter pylori infection and cap polyposis of the colon. Helicobacter. 2004; 9:651–656.12. Shimizu K, Koga H, Iida M, et al. Does metronidazole cure cap polyposis by its antiinflammatory actions instead of by its antibiotic action? A case study. Dig Dis Sci. 2002; 47:1465–1468.13. Kajihara H, Uno Y, Ying H, Tanaka M, Munakata A. Features of cap polyposis by magnifying colonoscopy. Gastrointest Endosc. 2000; 52:775–778.
Article14. Oiya H, Okawa K, Aoki T, Nebiki H, Inoue T. Cap polyposis cured by Helicobacter pylori eradication therapy. J Gastroenterol. 2002; 37:463–466.15. Ng KH, Mathur P, Kumarasinghe MP, Eu KW, Seow-Choen F. Cap polyposis: further experience and review. Dis Colon Rectum. 2004; 47:1208–1215.
Article16. Konishi T, Watanabe T, Takei Y, Kojima T, Nagawa H. Confined progression of cap polyposis along the anastomotic line, im-plicating the role of inflammatory responses in the pathogenesis. Gastrointest Endosc. 2005; 62:446–447.
Article17. Kim ES, Jeen YT, Keum B, et al. Remission of cap polyposis maintained for more than three years after infliximab treatment. Gut Liver. 2009; 3:325–328.
Article18. van Bommel EF, Siemes C, Hak LE, van der Veer SJ, Hendriksz TR. Longterm renal and patient outcome in idiopathic retroperitoneal fibrosis treated with prednisone. Am J Kidney Dis. 2007; 49:615–625.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Idiopathic Retroperitoneal Fibrosis: Report of a Case
- Idiopathic Retroperitoneal Fibrosis Treated with High Dose Steroids
- A Case of Idiopathic Retroperitoneal Fibrosis Treated by Bilateral Pyeloileoneocystostomy
- A Case of Idiopathic Retroperitoneal Fibrosis Associated with Rapidly Progressive Glomerulonephritis with Anti-myeloperoxidase Antineutrophil Cytoplasmic Antibodies
- Idiopathic Retroperitoneal Fibrosis Associated with a Horseshoe Kidney
