Yonsei Med J.
2016 Sep;57(5):1106-1114. 10.3349/ymj.2016.57.5.1106.
Long-Term Outcome and Surveillance Colonoscopy after Successful Endoscopic Treatment of Large Sessile Colorectal Polyps
- Affiliations
-
- 1Department of Medicine, Graduate School, Yonsei University College of Medicine, Seoul, Korea.
- 2Center for Cancer Prevention and Detection, National Cancer Center, Goyang, Korea.
- 3Department of Internal Medicine, Institute of Gastroenterology, Yonsei University College of Medicine, Seoul, Korea. sphong@yuhs.ac
- KMID: 2374154
- DOI: http://doi.org/10.3349/ymj.2016.57.5.1106
Abstract
- PURPOSE
Although there is a consensus about the need for surveillance colonoscopy after endoscopic resection, the interval remains controversial for large sessile colorectal polyps. The aim of this study was to evaluate the long-term outcome and the adequate surveillance colonoscopy interval required for sessile and flat colorectal polyps larger than 20 mm.
MATERIALS AND METHODS
A total of 204 patients with large sessile and flat polyps who received endoscopic treatment from May 2005 to November 2011 in a tertiary referral center were included.
RESULTS
The mean age was 65.1 years and 62.7% of the patients were male. The mean follow-up duration was 44.2 months and the median tumor size was 25 mm. One hundred and ten patients (53.9%) received a short interval surveillance colonoscopy (median interval of 6.3 months with range of 1-11 months) and 94 patients (46.1%) received a long interval surveillance colonoscopy (median interval of 13.6 months with range of 12-66 months). There were 14 patients (6.9%) who had local recurrence at the surveillance colonoscopy. Using multivariate regression analysis, a polyp size greater than 40 mm was shown to be independent risk factor for local recurrence. However, piecemeal resection and surveillance colonoscopy interval did not significantly influence local recurrence.
CONCLUSION
Endoscopic treatment of large sessile colorectal polyps shows a favorable long-term outcome. Further prospective study is mandatory to define an adequate interval of surveillance colonoscopy.
MeSH Terms
Figure
-
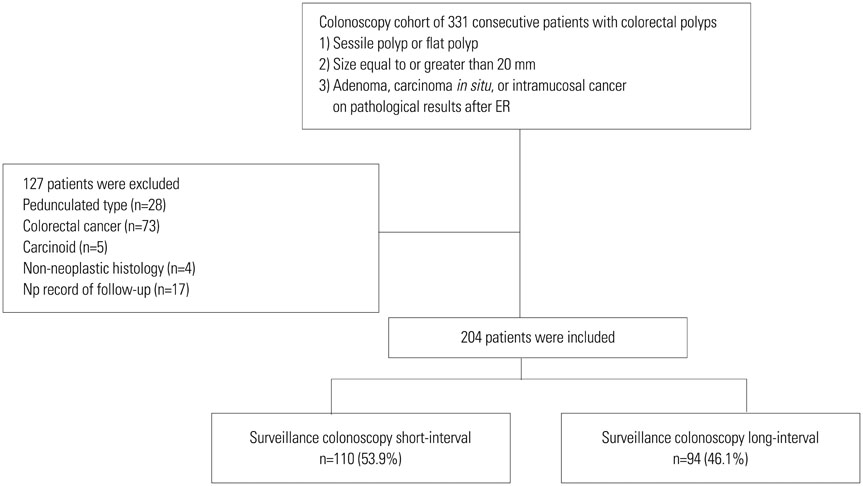
Fig. 1 Flow chart of patients throughout the study. We excluded colorectal tumors with stalks, colorectal cancers, carcinoids, tumors with a non-neoplastic histology, or patients without follow-up colonoscopy. Among the 331 consecutive patients, a total of 127 patients were excluded for the following reasons: pedunculated type (n=28), colorectal cancer (n=73), carcinoid (n=5), non-neoplastic histology (n=4), and no record of follow-up colonoscopy (n=17).
Reference
-
1. Luigiano C, Consolo P, Scaffidi MG, Strangio G, Giacobbe G, Alibrandi A, et al. Endoscopic mucosal resection for large and giant sessile and flat colorectal polyps: a single-center experience with long-term follow-up. Endoscopy. 2009; 41:829–835.
Article2. Conio M, Repici A, Demarquay JF, Blanchi S, Dumas R, Filiberti R. EMR of large sessile colorectal polyps. Gastrointest Endosc. 2004; 60:234–241.
Article3. Fukami N, Lee JH. Endoscopic treatment of large sessile and flat colorectal lesions. Curr Opin Gastroenterol. 2006; 22:54–59.
Article4. Brooker JC, Saunders BP, Shah SG, Thapar CJ, Suzuki N, Williams CB. Treatment with argon plasma coagulation reduces recurrence after piecemeal resection of large sessile colonic polyps: a randomized trial and recommendations. Gastrointest Endosc. 2002; 55:371–375.
Article5. Jang HW, Park SJ, Cheon JH, Kim TI, Kim WH, Hong SP. Does magnifying narrow-band imaging or magnifying chromoendoscopy help experienced endoscopists assess invasion depth of large sessile and flat polyps? Dig Dis Sci. 2014; 59:1520–1528.
Article6. Moss A, Bourke MJ, Williams SJ, Hourigan LF, Brown G, Tam W, et al. Endoscopic mucosal resection outcomes and prediction of submucosal cancer from advanced colonic mucosal neoplasia. Gastroenterology. 2011; 140:1909–1918.
Article7. Tajika M, Niwa Y, Bhatia V, Kondo S, Tanaka T, Mizuno N, et al. Comparison of endoscopic submucosal dissection and endoscopic mucosal resection for large colorectal tumors. Eur J Gastroenterol Hepatol. 2011; 23:1042–1049.
Article8. Kobayashi N, Saito Y, Uraoka T, Matsuda T, Suzuki H, Fujii T. Treatment strategy for laterally spreading tumors in Japan: before and after the introduction of endoscopic submucosal dissection. J Gastroenterol Hepatol. 2009; 24:1387–1392.
Article9. Lee EJ, Lee JB, Lee SH, Youk EG. Endoscopic treatment of large colorectal tumors: comparison of endoscopic mucosal resection, endoscopic mucosal resection-precutting, and endoscopic submucosal dissection. Surg Endosc. 2012; 26:2220–2230.
Article10. Katsinelos P, Kountouras J, Paroutoglou G, Zavos C, Rizos C, Beltsis A. Endoscopic mucosal resection of large sessile colorectal polyps with submucosal injection of hypertonic 50 percent dextrose-epinephrine solution. Dis Colon Rectum. 2006; 49:1384–1392.
Article11. Sakamoto T, Matsuda T, Otake Y, Nakajima T, Saito Y. Predictive factors of local recurrence after endoscopic piecemeal mucosal resection. J Gastroenterol. 2012; 47:635–640.
Article12. Winawer SJ, Zauber AG, Fletcher RH, Stillman JS, O'Brien MJ, Levin B, et al. Guidelines for colonoscopy surveillance after polypectomy: a consensus update by the US Multi-Society Task Force on Colorectal Cancer and the American Cancer Society. Gastroenterology. 2006; 130:1872–1885.
Article13. Bond JH. Polyp guideline: diagnosis, treatment, and surveillance for patients with colorectal polyps. Practice Parameters Committee of the American College of Gastroenterology. Am J Gastroenterol. 2000; 95:3053–3063.
Article14. Davila RE, Rajan E, Baron TH, Adler DG, Egan JV, Faigel DO, et al. ASGE guideline: colorectal cancer screening and surveillance. Gastrointest Endosc. 2006; 63:546–557.
Article15. Atkin WS, Saunders BP. British Society for Gastroenterology. Association of Coloproctology for Great Britain and Ireland. Surveillance guidelines after removal of colorectal adenomatous polyps. Gut. 2002; 51:Suppl 5. V6–V9.
Article16. Hurlstone DP, Sanders DS, Cross SS, Adam I, Shorthouse AJ, Brown S, et al. Colonoscopic resection of lateral spreading tumours: a prospective analysis of endoscopic mucosal resection. Gut. 2004; 53:1334–1339.
Article17. Yamamoto H, Kawata H, Sunada K, Sasaki A, Nakazawa K, Miyata T, et al. Successful en-bloc resection of large superficial tumors in the stomach and colon using sodium hyaluronate and small-caliber-tip transparent hood. Endoscopy. 2003; 35:690–694.
Article18. Lee SH, Chung IK, Kim SJ, Kim JO, Ko BM, Kim WH, et al. Comparison of postpolypectomy bleeding between epinephrine and saline submucosal injection for large colon polyps by conventional polypectomy: a prospective randomized, multicenter study. World J Gastroenterol. 2007; 13:2973–2977.
Article19. Ishii N, Itoh T, Horiki N, Matsuda M, Setoyama T, Suzuki S, et al. Endoscopic submucosal dissection with a combination of small-caliber-tip transparent hood and flex knife for large superficial colorectal neoplasias including ileocecal lesions. Surg Endosc. 2010; 24:1941–1947.
Article20. Saito Y, Uraoka T, Yamaguchi Y, Hotta K, Sakamoto N, Ikematsu H, et al. A prospective, multicenter study of 1111 colorectal endoscopic submucosal dissections (with video). Gastrointest Endosc. 2010; 72:1217–1225.
Article21. Fujishiro M, Yahagi N, Nakamura M, Kakushima N, Kodashima S, Ono S, et al. Endoscopic submucosal dissection for rectal epithelial neoplasia. Endoscopy. 2006; 38:493–497.
Article22. Rex DK, Bond JH, Winawer S, Levin TR, Burt RW, Johnson DA, et al. Quality in the technical performance of colonoscopy and the continuous quality improvement process for colonoscopy: recommendations of the U.S. Multi-Society Task Force on Colorectal Cancer. Am J Gastroenterol. 2002; 97:1296–1308.
Article23. Benedix F, Kube R, Meyer F, Schmidt U, Gastinger I, Lippert H, et al. Comparison of 17,641 patients with right- and left-sided colon cancer: differences in epidemiology, perioperative course, histology, and survival. Dis Colon Rectum. 2010; 53:57–64.
Article24. Suttie SA, Shaikh I, Mullen R, Amin AI, Daniel T, Yalamarthi S. Outcome of right- and left-sided colonic and rectal cancer following surgical resection. Colorectal Dis. 2011; 13:884–889.
Article25. Consolo P, Luigiano C, Strangio G, Scaffidi MG, Giacobbe G, Di Giuseppe G, et al. Efficacy, risk factors and complications of endoscopic polypectomy: ten year experience at a single center. World J Gastroenterol. 2008; 14:2364–2369.
Article26. Lieberman DA, Rex DK, Winawer SJ, Giardiello FM, Johnson DA, Levin TR, et al. Guidelines for colonoscopy surveillance after screening and polypectomy: a consensus update by the US Multi-Society Task Force on Colorectal Cancer. Gastroenterology. 2012; 143:844–857.
Article27. Zlatanic J, Waye JD, Kim PS, Baiocco PJ, Gleim GW. Large sessile colonic adenomas: use of argon plasma coagulator to supplement piecemeal snare polypectomy. Gastrointest Endosc. 1999; 49:731–735.
Article28. He L, Deng T, Luo H. Efficacy and safety of endoscopic resection therapies for rectal carcinoid tumors: a meta-analysis. Yonsei Med J. 2015; 56:72–81.
Article29. Moss A, Williams SJ, Hourigan LF, Brown G, Tam W, Singh R, et al. Long-term adenoma recurrence following wide-field endoscopic mucosal resection (WF-EMR) for advanced colonic mucosal neoplasia is infrequent: results and risk factors in 1000 cases from the Australian Colonic EMR (ACE) study. Gut. 2015; 64:57–65.
Article30. Knabe M, Pohl J, Gerges C, Ell C, Neuhaus H, Schumacher B. Standardized long-term follow-up after endoscopic resection of large, nonpedunculated colorectal lesions: a prospective two-center study. Am J Gastroenterol. 2014; 109:183–189.
Article31. Lee S, Park SJ, Cheon JH, Kim TI, Kim WH, Kang DR, et al. Child-Pugh score is an independent risk factor for immediate bleeding after colonoscopic polypectomy in liver cirrhosis. Yonsei Med J. 2014; 55:1281–1288.
Article32. Yang DH, Hong SN, Kim YH, Hong SP, Shin SJ, Kim SE, et al. Korean guidelines for postpolypectomy colonoscopy surveillance. Clin Endosc. 2012; 45:44–61.
Article33. Jang HW, Park SJ, Hong SP, Cheon JH, Kim WH, Kim TI. Risk factors for recurrent high-risk polyps after the removal of high-risk polyps at initial colonoscopy. Yonsei Med J. 2015; 56:1559–1565.
Article34. Kim YJ, Kim ES, Cho KB, Park KS, Jang BK, Chung WJ, et al. Comparison of clinical outcomes among different endoscopic resection methods for treating colorectal neoplasia. Dig Dis Sci. 2013; 58:1727–1736.
Article35. Carvalho R, Areia M, Brito D, Saraiva S, Alves S, Cadime AT. Endoscopic mucosal resection of large colorectal polyps: prospective evaluation of recurrence and complications. Acta Gastroenterol Belg. 2013; 76:225–230.36. Probst A, Golger D, Anthuber M, Märkl B, Messmann H. Endoscopic submucosal dissection in large sessile lesions of the rectosigmoid: learning curve in a European center. Endoscopy. 2012; 44:660–667.
Article37. Wang J, Zhang XH, Ge J, Yang CM, Liu JY, Zhao SL. Endoscopic submucosal dissection vs endoscopic mucosal resection for colorectal tumors: a meta-analysis. World J Gastroenterol. 2014; 20:8282–8287.
Article38. Hotta K, Fujii T, Saito Y, Matsuda T. Local recurrence after endoscopic resection of colorectal tumors. Int J Colorectal Dis. 2009; 24:225–230.
Article39. Saito Y, Sakamoto T, Fukunaga S, Nakajima T, Kiriyama S, Matsuda T. Endoscopic submucosal dissection (ESD) for colorectal tumors. Dig Endosc. 2009; 21:Suppl 1. S7–S12.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Optimal Colonoscopy Surveillance Interval after Polypectomy
- Strategy for post-polypectomy colonoscopy surveillance: focus on the revised Korean guidelines
- Characteristics and outcomes of endoscopically resected colorectal cancers that arose from sessile serrated adenomas and traditional serrated adenomas
- Should We Resect and Discard Low Risk Diminutive Colon Polyps
- Practice Patterns of Colorectal Polypectomy in Pediatric Endoscopic Specialists in South Korea: A Nationwide Survey Study
