Yonsei Med J.
2016 Jul;57(4):831-839. 10.3349/ymj.2016.57.4.831.
Fibroblast Growth Factor Receptor 1 Overexpression Is Associated with Poor Survival in Patients with Resected Muscle Invasive Urothelial Carcinoma
- Affiliations
-
- 1Department of Internal Medicine, Wonju Severance Christian Hospital, Wonju, Korea.
- 2Department of Medicine, Graduate School of Yonsei University College of Medicine, Seoul, Korea. rha7655@yuhs.ac
- 3Department of Pathology, Daedong Hospital, Busan, Korea.
- 4Department of Pathology, Yonsei University College of Medicine, Seoul, Korea.
- 5Department of Urology, Yonsei University College of Medicine, Seoul, Korea.
- 6Yonsei Cancer Center, Yonsei University Health System, Seoul, Korea.
- 7Department of Hematology and Oncology, Konyang University College of Medicine, Daejeon, Korea.
- 8Department of Pharmacology, Myunggok Medical Research Institute, College of Medicine, Konyang University, Daejeon, Korea.
- 9Division of Medical Oncology, Department of Internal Medicine, Yonsei University College of Medicine, Seoul, Korea.
- 10Song-Dang Institute for Cancer Research, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 2374112
- DOI: http://doi.org/10.3349/ymj.2016.57.4.831
Abstract
- PURPOSE
To examine the usefulness of various receptor tyrosine kinase expressions as prognostic markers and therapeutic targets in muscle invasive urothelial cancer (UC) patients.
MATERIALS AND METHODS
We retrospectively analyzed the data of 98 patients with muscle invasive UC who underwent radical cystectomy between 2005 and 2010 in Yonsei Cancer Center. Using formalin fixed paraffin embedded tissues of primary tumors, immunohistochemical staining was done for human epidermal growth factor receptor 2 (HER2), fibroblast growth factor receptor 1 (FGFR1), and fibroblast growth factor receptor 3 (FGFR3).
RESULTS
There were 41 (41.8%), 44 (44.9%), and 14 (14.2%) patients who have over-expressed HER2, FGFR1, and FGFR3, respectively. In univariate analysis, significantly shorter median time to recurrence (TTR) (12.9 months vs. 49.0 months; p=0.008) and overall survival (OS) (22.3 months vs. 52.7 months; p=0.006) was found in patients with FGFR1 overexpression. By contrast, there was no difference in TTR or OS according to the HER2 and FGFR3 expression status. FGFR1 remained as a significant prognostic factor for OS with hazard ratio of 2.23 (95% confidence interval: 1.27-3.90, p=0.006) in multivariate analysis.
CONCLUSION
Our result showed that FGFR1 expression, but not FGFR3, is an adverse prognostic factor in muscle invasive UC patients after radical cystectomy. FGFR1 might be feasible for prognosis prediction and a potential therapeutic target after thorough validation in muscle invasive UC.
MeSH Terms
-
Adult
Aged
Aged, 80 and over
Carcinoma/*metabolism/*mortality/surgery
Cystectomy
Female
Humans
Male
Middle Aged
Multivariate Analysis
Muscles/pathology
Neoplasm Invasiveness
Prognosis
Proportional Hazards Models
Receptor, ErbB-2/metabolism
Receptor, Fibroblast Growth Factor, Type 1/*metabolism
Receptor, Fibroblast Growth Factor, Type 3/metabolism
Retrospective Studies
Survival Rate
Urinary Bladder Neoplasms/*metabolism/*mortality/surgery
Urothelium/pathology
Receptor, ErbB-2
Receptor, Fibroblast Growth Factor, Type 1
Receptor, Fibroblast Growth Factor, Type 3
Figure
-
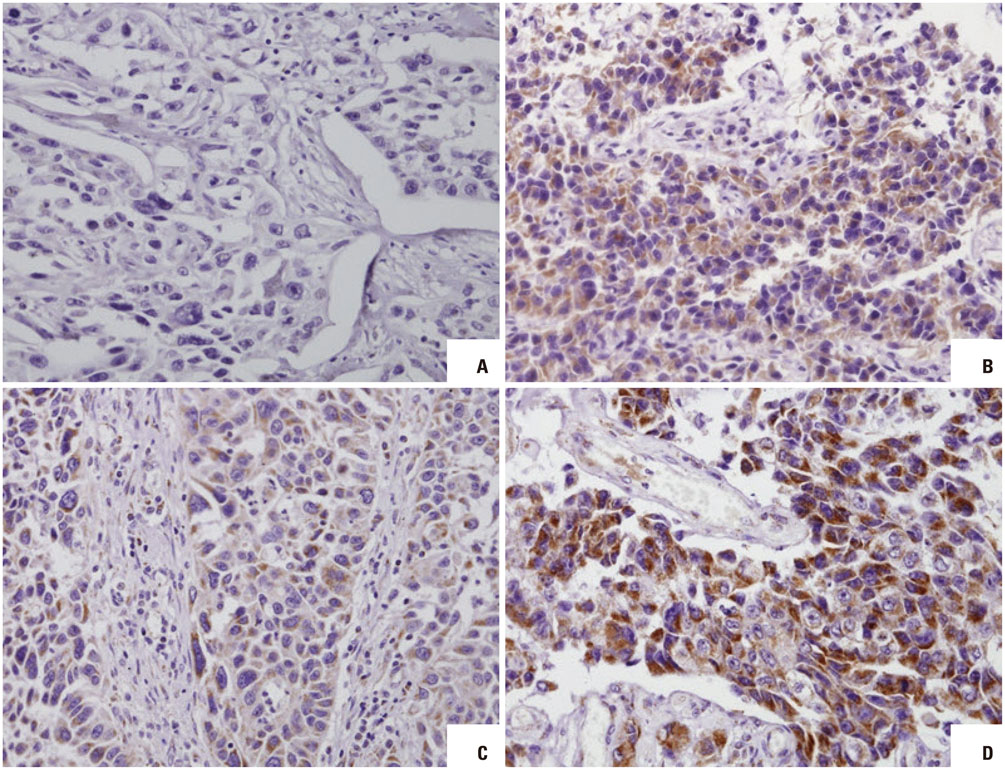
Fig. 1 Immunohistochemistry staining (×200) of urothelial carcinoma showing different grades of FGFR1 expression. (A) Negative. (B) Moderate signaling in 30% of cells. (C) Weak signaling in 70% of cells. (D) Moderate signaling in 70% of cells. FGFR1, fibroblast growth factor receptor 1.
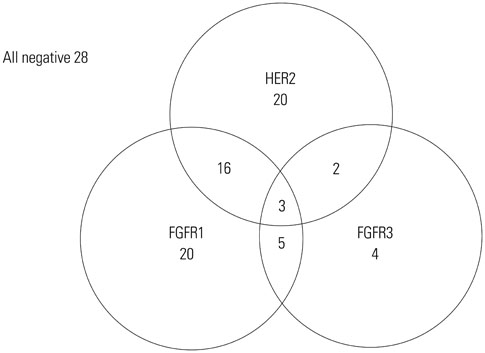
Fig. 2 Distribution of patients according to the HER2 and FGFR expression status. HER2, human epidermal growth factor receptor 2; FGFR, fibroblast growth factor receptor.

Fig. 3 Survival curves according to FGFR1 expression level. (A) Progression free survival. (B) Overall survival. FGFR1, fibroblast growth factor receptor 1.
Reference
-
1. Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin. 2015; 65:87–108.
Article2. Knowles MA. Molecular subtypes of bladder cancer: Jekyll and Hyde or chalk and cheese? Carcinogenesis. 2006; 27:361–373.
Article3. Wu XR. Urothelial tumorigenesis: a tale of divergent pathways. Nat Rev Cancer. 2005; 5:713–725.
Article4. Stein JP, Lieskovsky G, Cote R, Groshen S, Feng AC, Boyd S, et al. Radical cystectomy in the treatment of invasive bladder cancer: long-term results in 1,054 patients. J Clin Oncol. 2001; 19:666–675.
Article5. von der Maase H, Hansen SW, Roberts JT, Dogliotti L, Oliver T, Moore MJ, et al. Gemcitabine and cisplatin versus methotrexate, vinblastine, doxorubicin, and cisplatin in advanced or metastatic bladder cancer: results of a large, randomized, multinational, multicenter, phase III study. J Clin Oncol. 2000; 18:3068–3077.
Article6. Slamon DJ, Leyland-Jones B, Shak S, Fuchs H, Paton V, Bajamonde A, et al. Use of chemotherapy plus a monoclonal antibody against HER2 for metastatic breast cancer that overexpresses HER2. N Engl J Med. 2001; 344:783–792.
Article7. Romond EH, Perez EA, Bryant J, Suman VJ, Geyer CE Jr, Davidson NE, et al. Trastuzumab plus adjuvant chemotherapy for operable HER2-positive breast cancer. N Engl J Med. 2005; 353:1673–1684.
Article8. Bang YJ, Van Cutsem E, Feyereislova A, Chung HC, Shen L, Sawaki A, et al. Trastuzumab in combination with chemotherapy versus chemotherapy alone for treatment of HER2-positive advanced gastric or gastro-oesophageal junction cancer (ToGA): a phase 3, open-label, randomised controlled trial. Lancet. 2010; 376:687–697.
Article9. Laé M, Couturier J, Oudard S, Radvanyi F, Beuzeboc P, Vieillefond A. Assessing HER2 gene amplification as a potential target for therapy in invasive urothelial bladder cancer with a standardized methodology: results in 1005 patients. Ann Oncol. 2010; 21:815–819.
Article10. Marín AP, Arranz EE, Sánchez AR, Auñón PZ, Barón MG. Role of anti-Her-2 therapy in bladder carcinoma. J Cancer Res Clin Oncol. 2010; 136:1915–1920.
Article11. Mellon JK, Lunec J, Wright C, Horne CH, Kelly P, Neal DE. CerbB-2 in bladder cancer: molecular biology, correlation with epidermal growth factor receptors and prognostic value. J Urol. 1996; 155:321–326.
Article12. Lönn U, Lönn S, Friberg S, Nilsson B, Silfverswärd C, Stenkvist B. Prognostic value of amplification of c-erb-B2 in bladder carcinoma. Clin Cancer Res. 1995; 1:1189–1194.13. Vollmer RT, Humphrey PA, Swanson PE, Wick MR, Hudson ML. Invasion of the bladder by transitional cell carcinoma: its relation to histologic grade and expression of p53, MIB-1, c-erb B-2, epidermal growth factor receptor, and bcl-2. Cancer. 1998; 82:715–723.
Article14. Kolla SB, Seth A, Singh MK, Gupta NP, Hemal AK, Dogra PN, et al. Prognostic significance of Her2/neu overexpression in patients with muscle invasive urinary bladder cancer treated with radical cystectomy. Int Urol Nephrol. 2008; 40:321–327.
Article15. L'Hôte CG, Knowles MA. Cell responses to FGFR3 signalling: growth, differentiation and apoptosis. Exp Cell Res. 2005; 304:417–431.16. di Martino E, Tomlinson DC, Knowles MA. A decade of FGF receptor research in bladder cancer: past, present, and future challenges. Adv Urol. 2012; 2012:429213.
Article17. Ornitz DM, Itoh N. Fibroblast growth factors. Genome Biol. 2001; 2:REVIEWS3005.18. Tomlinson DC, Baldo O, Harnden P, Knowles MA. FGFR3 protein expression and its relationship to mutation status and prognostic variables in bladder cancer. J Pathol. 2007; 213:91–98.
Article19. Lamont FR, Tomlinson DC, Cooper PA, Shnyder SD, Chester JD, Knowles MA. Small molecule FGF receptor inhibitors block FGFR-dependent urothelial carcinoma growth in vitro and in vivo. Br J Cancer. 2011; 104:75–82.
Article20. Tomlinson DC, Lamont FR, Shnyder SD, Knowles MA. Fibroblast growth factor receptor 1 promotes proliferation and survival via activation of the mitogen-activated protein kinase pathway in bladder cancer. Cancer Res. 2009; 69:4613–4620.
Article21. Edge S, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A. AJCC cancer staging manual. 7th ed. New York: Springer;2010.22. Kim HR, Kim DJ, Kang DR, Lee JG, Lim SM, Lee CY, et al. Fibroblast growth factor receptor 1 gene amplification is associated with poor survival and cigarette smoking dosage in patients with resected squamous cell lung cancer. J Clin Oncol. 2013; 31:731–737.
Article23. Jung EJ, Jung EJ, Min SY, Kim MA, Kim WH. Fibroblast growth factor receptor 2 gene amplification status and its clinicopathologic significance in gastric carcinoma. Hum Pathol. 2012; 43:1559–1566.
Article24. Jang M, Kim E, Choi Y, Lee H, Kim Y, Kim J, et al. FGFR1 is amplified during the progression of in situ to invasive breast carcinoma. Breast Cancer Res. 2012; 14:R115.25. Tomlinson DC, Knowles MA. Altered splicing of FGFR1 is associated with high tumor grade and stage and leads to increased sensitivity to FGF1 in bladder cancer. Am J Pathol. 2010; 177:2379–2386.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Expression of Fibroblast Growth Factor Receptor 3 in the Recurrence of Non-Muscle-Invasive Urothelial Carcinoma of the Bladder
- Pronostic Value of The Expression of Mutant p53 and EGFR mRNA in Transitional Cell Carcinoma of the Bladder
- The Role of Fibroblast Growth Factor Receptors Inhibitors in Bladder Cancer
- VEGF and Ki-67 Overexpression in Predicting Poor Overall Survival in Adenoid Cystic Carcinoma
- Pfeiffer Syndrome Type 2 with Sporadic Fibroblast Growth Factor Receptor 2 Mutation and Coccygeal Anomaly
