Incipient Ocular Mucosa-associated Lymphoid Tissue Lymphoma in IgG4-related Orbital Disease
- Affiliations
-
- 1Institute of Vision Research, Department of Ophthalmology, Yonsei University College of Medicine, Seoul, Korea.
- 2Kyung Hee University College of Medicine, Seoul, Korea.
- 3Department of Ophthalmology, Kyungpook National University School of Medicine, Daegu, Korea.
- 4Department of Pathology, Yonsei University College of Medicine, Seoul, Korea.
- 5Institute of Vision Research, Department of Ophthalmology, Yonsei University College of Medicine, Seoul, Korea. yoonjs@yuhs.ac
- KMID: 2373475
- DOI: http://doi.org/10.3341/kjo.2017.31.2.172
Abstract
- No abstract available.
Figure
-
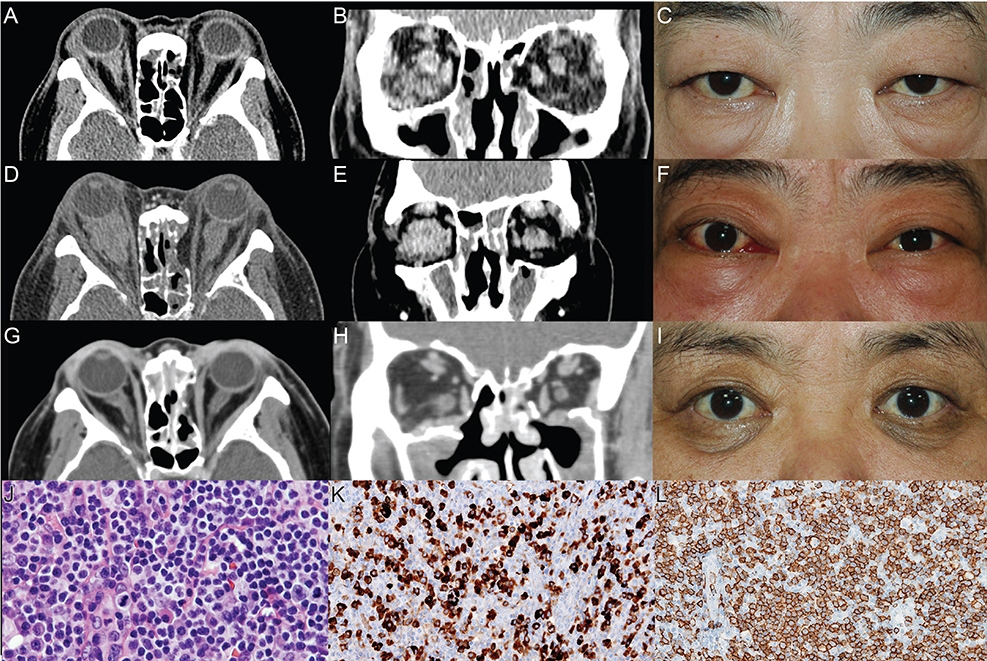
Fig. 1 (A,B) Initial computed tomography (CT) shows diffuse thickening of the extraocular muscles and a dense retrobulbar infiltration around the optic nerve that is more severe in the right eye than the left eye. (C) Bilateral periorbital swelling is shown. (D,E) Preoperative CT shows an increase in the size of the lobulated mass in the bilateral orbit and retrobulbar area and diffuse enlargement of the bilateral infraorbital nerve and bilateral superior rectus muscles. Additionally, a slight increase in the size of the bilateral lacrimal glands and bilateral paranasal sinusitis are shown. (F) Signs of inflammation, such as conjunctival injection, caruncle injection and swelling, proptosis, and periorbital swelling are apparent. (G,H) Three months after debulking surgery, CT shows a much decreased size of the retrobulbar mass, thickening of the extraocular muscles, and improvement in the dense retrobulbar infiltration. Moreover, the increased volume of the orbital cavity, owing to medial and inferior orbital wall decompression surgery, is shown. (I) Proptosis and periorbital swelling show improvement and there are no signs of inflammation. (J) Hematoxylin and eosin staining reveals monomorphous small-to-medium-size lymphoid cells and plasma cells without significant atypia (×100). (K) Immunohistochemical staining reveals mild perifollicular expansion of CD20+ B-cells (×100). (L) Immunostaining of IgG4 shows many IgG4-positive plasma cells with a high ratio of IgG4-positive plasma cells: IgG-positive plasma cells (~60%) (×200).
Reference
-
1. van den Brand M, van Krieken JH. Recognizing nodal marginal zone lymphoma: recent advances and pitfalls. A systematic review. Haematologica. 2013; 98:1003–1013.2. Lee MJ, Kim N, Choe JY, et al. Clinicopathological analysis of ocular adnexal extranodal marginal zone B-cell lymphoma with IgG4-positive cells. PLoS One. 2015; 10:e0131458.3. Igawa T, Hayashi T, Ishiguro K, et al. IgG4-producing lymphoma arising in a patient with IgG4-related disease. Med Mol Morphol. 2016; 49:243–249.4. Yamamoto M, Takahashi H, Tabeya T, et al. Risk of malignancies in IgG4-related disease. Mod Rheumatol. 2012; 22:414–418.5. Umehara H, Okazaki K, Masaki Y, et al. Comprehensive diagnostic criteria for IgG4-related disease (IgG4-RD), 2011. Mod Rheumatol. 2012; 22:21–30.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Ocular adnexal mucosa-associated lymphoid tissue lymphoma: a narrative review
- The Prognosis of Ocular-adnexal Lymphoproliferative Lesions
- Mucosa-Associated Lymphoid Tissue Lymphoma of the Esophagus Coexistent with Bronchus-Associated Lymphoid Tissue Lymphoma of the Lung
- A case report of the Pulmonary Malignant Lymphomaof the mucosa-associated lymphoid tissue(MALT)
- Role of Chemotherapy in Gastric Marginal Zone B-Cell Lymphoma of Mucosa-Associated Lymphoid Tissue (MALT) Type
