A Case of Advanced Gastric Cancer with Para-Aortic Lymph Node Metastasis from Co-Occurring Prostate Cancer
- Affiliations
-
- 1Department of Anesthesiology, Gyeongsang National University School of Medicine, Jinju, Korea.
- 2Department of Surgery, Gyeongsang National University School of Medicine, Jinju, Korea. jshgnu@gmail.com
- 3Department of Pathology, Gyeongsang National University School of Medicine, Jinju, Korea.
- KMID: 2372586
- DOI: http://doi.org/10.5230/jgc.2017.17.e10
Abstract
- An 84-year-old man was diagnosed with two synchronous adenocarcinomas, a Borrmann type IV advanced gastric adenocarcinoma in his antrum and a well-differentiated Borrmann type I carcinoma on the anterior wall of the higher body of his stomach. Pre-operatively, computed tomography of the abdomen revealed the presence of advanced gastric cancer with peri-gastric and para-aortic lymph node (LN) metastasis. He planned for palliative total gastrectomy owing to the risk of obstruction by the antral lesion. We performed a frozen biopsy of a para-aortic LN during surgery and found that the origin of the para-aortic LN metastasis was from undiagnosed prostate cancer. Thus, we performed radical total gastrectomy and D2 LN dissection. Post-operatively, his total prostate-specific antigen levels were high (227 ng/mL) and he was discharged 8 days after surgery without any complications.
MeSH Terms
Figure
-
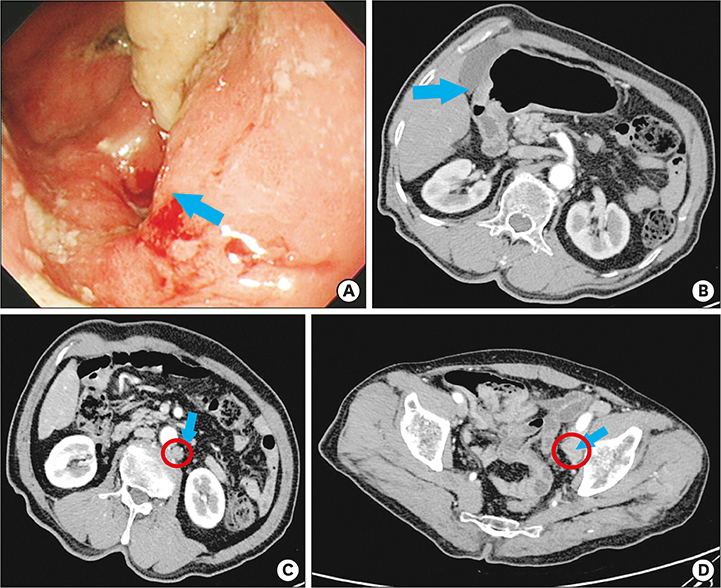
Fig. 1 (A) Gastrofibroscopic findings indicate a pyloric canal that is nearly obstructed by an encircling cancer mass (blue arrow). (B) Wall thickness in the pyloric area was found on a CT scan (blue arrow). (C) Enlarged LNs in left para-aortic area (red ring). (D) Enlarged LNs in left iliac area (red ring). CT = computed tomography; LN = lymph node.

Fig. 2 Pathologic findings of the preoperative endoscopic gastric biopsy and the frozen para-aortic lymph node. (A) The endoscopic specimen showed varied findings, from well-formed glands to solid sheets of tumor cells (H&E, ×100). (B) Even in the well-formed glands, mitosis was frequently noted (H&E, ×400). (C) In the sheets, the tumor cells were variable in size and shape and showed vesicular nuclei rather than uniform small round nuclei (H&E, ×400). (D) The para-aortic lymph node showed well-differentiated adenocarcinoma with a low nuclear-tocytoplasmic ratio and low cellular atypia (H&E, ×200). (E) The tumor cells are strongly positive for the anti-prostate specific antigen antibody (PSA, ×200).
Reference
-
1. Jung KW, Won YJ, Kong HJ, Oh CM, Seo HG, Lee JS. Cancer statistics in Korea: incidence, mortality, survival and prevalence in 2010. Cancer Res Treat. 2013; 45:1–14.2. Jeong O, Park YK. Clinicopathological features and surgical treatment of gastric cancer in South Korea: the results of 2009 nationwide survey on surgically treated gastric cancer patients. J Gastric Cancer. 2011; 11:69–77.3. Fujitani K, Yang HK, Mizusawa J, Kim YW, Terashima M, Han SU, REGATTA study investigators, et al. Gastrectomy plus chemotherapy versus chemotherapy alone for advanced gastric cancer with a single non-curable factor (REGATTA): a phase 3, randomised controlled trial. Lancet Oncol. 2016; 17:309–318.4. Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2014 (ver. 4). Gastric Cancer. 2017; 20:1–19.5. Deng JY, Liang H. Clinical significance of lymph node metastasis in gastric cancer. World J Gastroenterol. 2014; 20:3967–3975.6. Japanese Gastric Cancer Association. Japanese classification of gastric carcinoma: 3rd English edition. Gastric Cancer. 2011; 14:101–112.7. Cunningham D, Allum WH, Stenning SP, Thompson JN, Van de Velde CJ, Nicolson M, MAGIC Trial Participants, et al. Perioperative chemotherapy versus surgery alone for resectable gastroesophageal cancer. N Engl J Med. 2006; 355:11–20.8. Cheng L, Rao Q, Huang WB. [Recent advance in staging of prostate cancer]. Zhonghua Bing Li Xue Za Zhi. 2013; 42:351–354.9. Loh KP, Mohile SG, Kessler E, Fung C. Treatment of metastatic prostate cancer in older adults. Curr Oncol Rep. 2016; 18:63.10. Kumar S, Podratz KC, Bakkum-Gamez JN, Dowdy SC, Weaver AL, McGree ME, et al. Prospective assessment of the prevalence of pelvic, paraaortic and high paraaortic lymph node metastasis in endometrial cancer. Gynecol Oncol. 2014; 132:38–43.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Laparoscopy-assisted gastrectomy with para-aortic lymphadenectomy after palliative chemotherapy for advanced gastric cancer with isolated para-aortic lymph node metastasis
- Para-aortic Lymph Node Dissection in Gastric Cancer
- Laparoscopic para-aortic lymph node dissection for patients with primary colorectal cancer and clinically suspected para-aortic lymph nodes
- Laparoscopic Para-aortic Lymph Node Dissection in Patients with Gynecologic Malignancy
- Prognosis of the Patients Showing Metastasis to the Para-aortic or/and Supraclavicular Lymph Nodes at the Time of Diagnosis of Recurrence of the Cervical Cancer
