Benign Thyroid and Neck Lesions Mimicking Malignancy with False Positive Findings on Positron Emission Tomography-Computed Tomography
- Affiliations
-
- 1Department of Radiology, Soonchunhyang University Cheonan Hospital, Cheonan, Korea. taloo@hanmail.net
- 2Department of Nuclear Medicine, Soonchunhyang University Cheonan Hospital, Cheonan, Korea.
- 3Department of Surgery, Younsei Angelot Women's Clinic, Cheonan, Korea.
- KMID: 2367860
- DOI: http://doi.org/10.3348/jksr.2017.76.2.126
Abstract
- The increasing use of positron emission tomography-computed tomography (PET/CT) has led to the frequent detection of incidental thyroid and neck lesions with increased ¹â¸F-deoxyglucose (FDG) uptake. Although lesions with increased FDG uptake are commonly assumed to be malignant, benign lesions may also exhibit increased uptake. The purpose of this pictorial essay is to demonstrate that benign thyroid and neck lesions can produce false-positive findings on PET/CT, and to identify various difficulties in interpretation. It is crucial to be aware that differentiating between benign and malignant lesions is difficult in a considerable proportion of cases, when relying only on PET/CT findings. Correlation of PET/CT findings with additional imaging modalities is essential to avoid misdiagnosis.
MeSH Terms
Figure
-
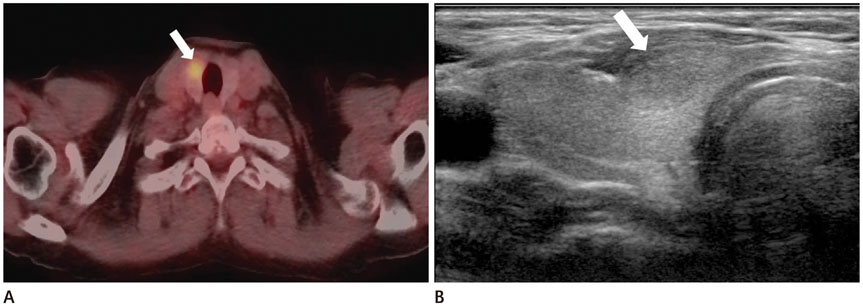
Fig. 1 Nodular hyperplasia, a 67-year-old woman with breast cancer. A. PET/CT transaxial fusion image shows focal FDG uptake in the right lobe of the thyroid gland (arrow) (SUVmax = 5.09). B. Ultrasonography image shows an oval shaped isoechoic nodule in the right thyroid lobe (arrow). FNA confirmed nodular hyperplasia. FDG = 18F-deoxyglucose, FNA = fine needle aspiration, PET/CT = positron emission tomography-computed tomography, SUV = standardized uptake value

Fig. 2 Hashimoto's thyroiditis, a 54-year-old woman, screening. A. PET/CT transaxial fusion image shows increased diffuse FDG uptake in both lobes of thyroid gland (arrows) (SUVmax = 4.2). B. Ultrasonography image shows heterogeneous parenchymal echogenicity with ill-defined oval hypoechoic nodules in the right lobe of the thyroid gland (arrow). FNA confirmed Hashimoto's thyroiditis. FDG = 18F-deoxyglucose, FNA = fine needle aspiration, PET/CT = positron emission tomography-computed tomography, SUV = standardized uptake value

Fig. 3 Subacute thyroiditis, a 62-year-old woman with stomach cancer. A. PET/CT transaxial fusion image shows increased diffuse FDG uptake in both lobes of the thyroid gland (arrows) (SUVmax = 3.47). B. Ultrasonography images show irregular margin and heterogeneous hypoechoic area in anterior portion of both lobes of the thyroid gland (arrows) with decreased vascularity on color Doppler ultrasonography (not shown). FNA confirmed subacute thyroiditis. FDG = 18F-deoxyglucose, FNA = fine needle aspiration, PET/CT = positron emission tomography-computed tomography, SUV = standardized uptake value
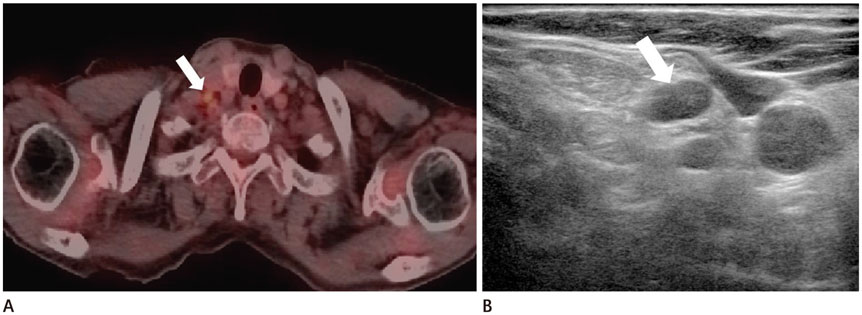
Fig. 4 Benign inflammation (tuberculous lymphadenopathy), a 75-year-old woman with cervical cancer. A. PET/CT transaxial fusion image shows increased focal nodular FDG uptake in right neck level IV (arrow) (SUVmax = 2.4). B. Ultrasonography image shows a small lymph node in the right neck with loss of fatty hilum (arrow). Biopsy confirmed tuberculosis. FDG = 18F-deoxyglucose, PET/CT = positron emission tomography-computed tomography, SUV = standardized uptake value
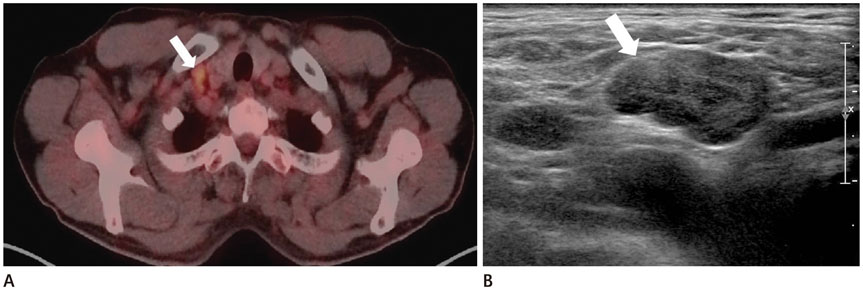
Fig. 5 Benign inflammation (reactive lymphadenopathy), a 69-year-old man with stomach cancer. A. PET/CT transaxial fusion image shows a lymph node in right supraclavicular area with increased FDG uptake (arrow) (SUVmax = 3.5). B. Ultrasonography image shows an enlarged lymph node in the right supraclavicular area with loss of fatty hilum (arrow). Biopsy confirmed reactive hyperplasia. FDG = 18F-deoxyglucose, PET/CT = positron emission tomography-computed tomography, SUV = standardized uptake value
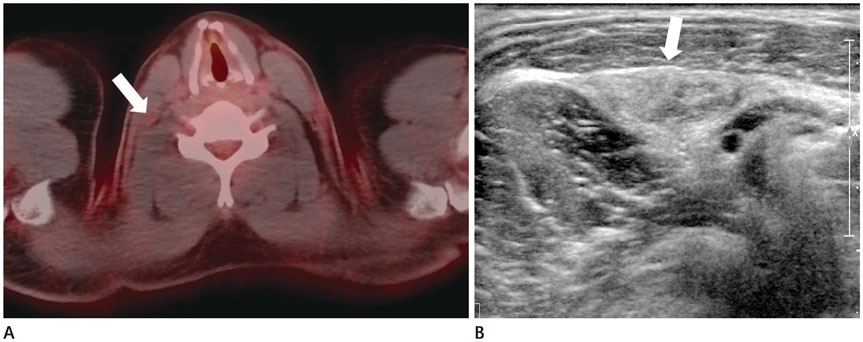
Fig. 6 Traumatic neuroma, a 32-year-old man with total thyroidectomy for papillary thyroid cancer. A. PET/CT transaxial fusion image shows increased FDG uptake in the right neck (arrow) (SUVmax = 2.1). B. Ultrasonography image shows a spindle-shaped circumscribed heterogeneous isoechoic nodule in the right neck (arrow). An 18G core needle biopsy was performed and traumatic neuroma was confirmed. FDG = 18F-deoxyglucose, PET/CT = positron emission tomography-computed tomography, SUV = standardized uptake value
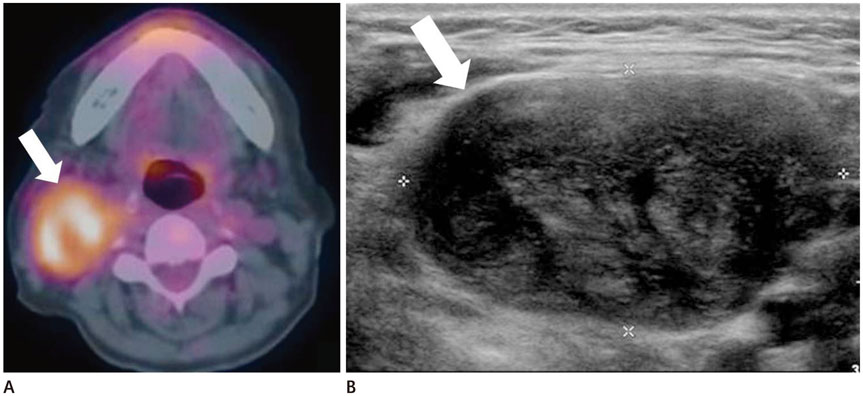
Fig. 7 Schwannoma, a 64-year-old woman with breast cancer. A. PET/CT transaxial fusion image shows increased focal nodular FDG uptake in the right neck (arrow) (SUVmax = 5.5). B. Ultrasonography image shows a circumscribed, oval, heterogeneous, hypoechoic nodule in the right neck (arrow). An 18G core needle biopsy confirmed schwannoma. FDG = 18F-deoxyglucose, PET/CT = positron emission tomography-computed tomography, SUV = standardized uptake value
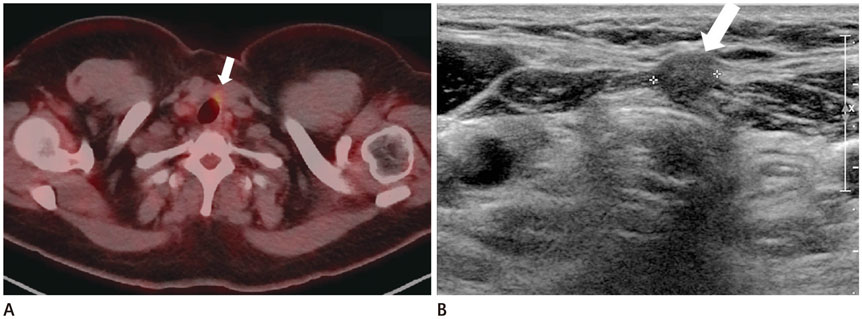
Fig. 8 Foreign body granuloma, a 43-year-old woman with left hemithyroidectomy for left thyroid cancer. A. PET/CT transaxial fusion image shows increased focal nodular FDG uptake in the postoperative bed of the left anterior neck (arrow) (SUVmax = 2.9). B. Ultrasonography image shows a well-defined, round, isoechoic nodular lesion in the postoperative bed of the left anterior neck (arrow). An 18G core needle biopsy was performed, confirming foreign body granuloma. FDG = 18F-deoxyglucose, PET/CT = positron emission tomography-computed tomography, SUV = standardized uptake value
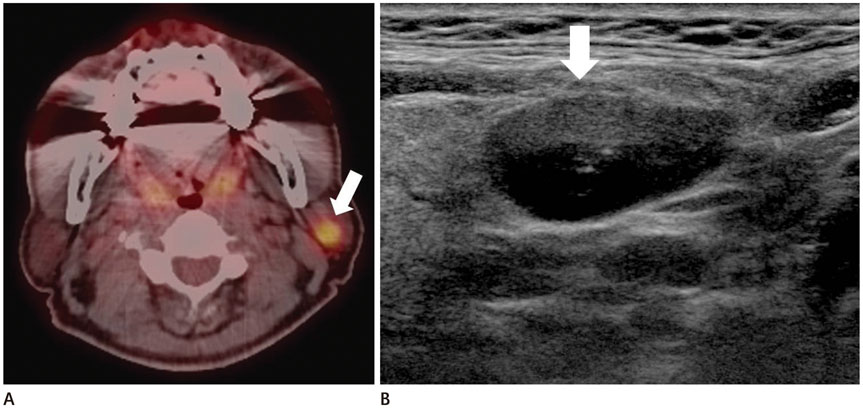
Fig. 9 Warthin's tumor, a 72-year-old man with supraglottic cancer. A. PET/CT transaxial fusion image shows increased focal nodular FDG uptake in the left parotid gland (arrow) (SUVmax=5.26). B. Ultrasonography image shows a well-defined, hypoechoic nodular lesion in the left parotid gland (arrow). An 18G core needle biopsy confirmed Warthin's tumor. FDG = 18F-deoxyglucose, PET/CT = positron emission tomography-computed tomography, SUV = standardized uptake value
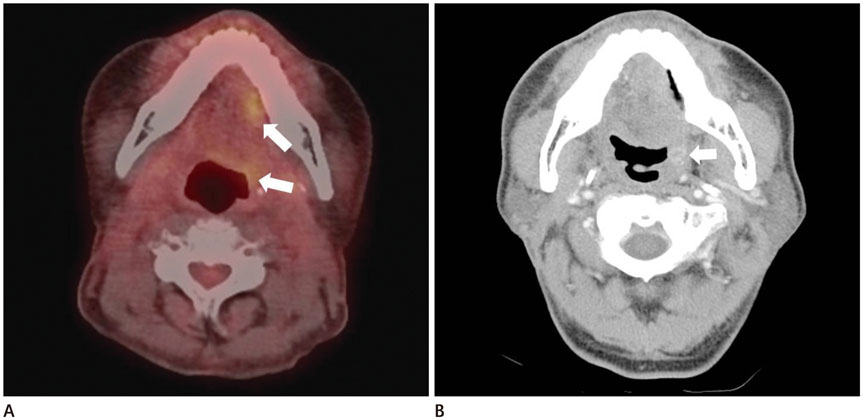
Fig. 10 Inflammation after recent surgery, a 55-year-old man following wide excision and chemoradiotherapy for tongue cancer. A. PET/CT transaxial fusion image shows focal FDG uptake in the operation bed and left oropharynx (arrows) (SUVmax = 4.1). B. Contrast-enhanced axial CT image shows a peripherally enhanced lesion in the left oropharynx (arrow). Physical examination and pathology confirmed the absence of malignancy. FDG = 18F-deoxyglucose, PET/CT = positron emission tomography-computed tomography, SUV = standardized uptake value

Fig. 11 Inflammation after radiotherapy, a 61-year-old man following radiotherapy for glottic cancer. A. Initial PET/CT transaxial fusion image shows no definite FDG uptake in the anterior neck muscles. B. A 10-month follow-up PET/CT transaxial fusion image shows a newly developed increased diffuse FDG uptake in the muscles of the anterior neck (arrows) (SUVmax = 3.05). FDG = 18F-deoxyglucose, PET/CT = positron emission tomography-computed tomography, SUV = standardized uptake value
Reference
-
1. Bae JS, Chae BJ, Park WC, Kim JS, Kim SH, Jung SS, et al. Incidental thyroid lesions detected by FDG-PET/CT: prevalence and risk of thyroid cancer. World J Surg Oncol. 2009; 7:63.2. Lee KH, Shin JH, Han BK, Ko EY, Ko ES, Hahn SY, et al. Incidental thyroid lesions detected on 18F-fluorodeoxyglucose positron emission tomography/CT in patients with non-thyroidal cancer: clinical implications and the value of ultrasound. J Korean Soc Radiol. 2014; 71:111–119.3. Purohit BS, Ailianou A, Dulguerov N, Becker CD, Ratib O, Becker M. FDG-PET/CT pitfalls in oncological head and neck imaging. Insights Imaging. 2014; 5:585–602.4. Fukui MB, Blodgett TM, Snyderman CH, Johnson JJ, Myers EN, Townsend DW, et al. Combined PET-CT in the head and neck: part 2. Diagnostic uses and pitfalls of oncologic imaging. Radiographics. 2005; 25:913–930.5. Solbiati L, Osti V, Cova L, Tonolini M. Ultrasound of thyroid, parathyroid glands and neck lymph nodes. Eur Radiol. 2001; 11:2411–2424.6. Yeo SH, Lee SK, Hwang I, Ahn EJ. Subacute thyroiditis presenting as a focal lesion on [18F] fluorodeoxyglucose whole-body positron-emission tomography/CT. AJNR Am J Neuroradiol. 2011; 32:E58–E60.7. Karantanis D, Bogsrud TV, Wiseman GA, Mullan BP, Subramaniam RM, Nathan MA, et al. Clinical significance of diffusely increased 18F-FDG uptake in the thyroid gland. J Nucl Med. 2007; 48:896–901.8. Liu Y, Ghesani NV, Zuckier LS. Physiology and pathophysiology of incidental findings detected on FDG-PET scintigraphy. Semin Nucl Med. 2010; 40:294–315.9. Skoura E, Zumla A, Bomanji J. Imaging in tuberculosis. Int J Infect Dis. 2015; 32:87–93.10. Vorster M, Sathekge MM, Bomanji J. Advances in imaging of tuberculosis: the role of 18F-FDG PET and PET/CT. Curr Opin Pulm Med. 2014; 20:287–293.11. Nair AV, Sandya CJ, Shagos GS, Anirudh S, Rajamma BM, Ramachandran PV, et al. Role of dual time fluorodeoxyglucose (FDG) positron emission tomography-computed tomography in identifying co-existing inflammatory and malignant disease: Who holds it (FDG) longer? Indian J Nucl Med. 2015; 30:139–141.12. Jacene HA, Stearns V, Wahl RL. Lymphadenopathy resulting from acute hepatitis C infection mimicking metastatic breast carcinoma on FDG PET/CT. Clin Nucl Med. 2006; 31:379–381.13. Payabvash S, Meric K, Cayci Z. Differentiation of benign from malignant cervical lymph nodes in patients with head and neck cancer using PET/CT imaging. Clin Imaging. 2016; 40:101–105.14. Yabuuchi H, Kuroiwa T, Fukuya T, Tomita K, Hachitanda Y. Traumatic neuroma and recurrent lymphadenopathy after neck dissection: comparison of radiologic features. Radiology. 2004; 233:523–529.15. Kim EY, Kang DK, Kim TH, Kim KS, Yim H. Traumatic neuroma in a breast cancer patient after modified radical mastectomy: a case report. J Korean Soc Radiol. 2011; 64:515–518.16. Liu Y. Orthopedic surgery-related benign uptake on FDG-PET: case examples and pitfalls. Ann Nucl Med. 2009; 23:701–708.17. Beaulieu S, Rubin B, Djang D, Conrad E, Turcotte E, Eary JF. Positron emission tomography of schwannomas: emphasizing its potential in preoperative planning. AJR Am J Roentgenol. 2004; 182:971–974.18. Anil G, Tan TY. Imaging characteristics of schwannoma of the cervical sympathetic chain: a review of 12 cases. AJNR Am J Neuroradiol. 2010; 31:1408–1412.19. Kim HR, Hong HS, Lee EH, Lee MH, Park JM, Kwak JJ, et al. Ultrasonographic findings of foreign-body granulomas after endoscopic thyroidectomy via an axillo-breast approach. J Korean Soc Radiol. 2012; 66:507–517.20. Miyake KK, Nakamoto Y, Mikami Y, Ishizu K, Saga T, Higashi T, et al. F-18 FDG PET of foreign body granuloma: pathologic correlation with imaging features in 3 cases. Clin Nucl Med. 2010; 35:853–857.21. Hadiprodjo D, Ryan T, Truong MT, Mercier G, Subramaniam RM. Parotid gland tumors: preliminary data for the value of FDG PET/CT diagnostic parameters. AJR Am J Roentgenol. 2012; 198:W185–W190.22. Uchida Y, Minoshima S, Kawata T, Motoori K, Nakano K, Kazama T, et al. Diagnostic value of FDG PET and salivary gland scintigraphy for parotid tumors. Clin Nucl Med. 2005; 30:170–176.23. Thoeny HC, De Keyzer F, King AD. Diffusion-weighted MR imaging in the head and neck. Radiology. 2012; 263:19–32.24. Ohba K, Sasaki S, Oki Y, Nishizawa S, Matsushita A, Yoshino A, et al. Factors associated with fluorine-18-fluorodeoxyglucose uptake in benign thyroid nodules. Endocr J. 2013; 60:985–990.25. Zochodne DW, Nguyen C, Sharkey KA. Accumulation and degranulation of mast cells in experimental neuromas. Neurosci Lett. 1994; 182:3–6.26. Horiuchi M, Yasuda S, Shohtsu A, Ide M. Four cases of Warthin’s tumor of the parotid gland detected with FDG PET. Ann Nucl Med. 1998; 12:47–50.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Transient ¹â¸F-Fluorodeoxyglucose Activity on PET/CT of Herniation Pit in Thyroid Cancer Patient: A Case Report
- Clinical Etiology of Hypermetabolic Pelvic Lesions in Postoperative Positron Emission Tomography/Computed Tomography for Patients With Rectal and Sigmoid Cancer
- False Positive and False Negative FDG-PET Scans in Various Thoracic Diseases
- 18F-2-Deoxy-2-Fluoro-D-Glucose Positron Emission Tomography: Computed Tomography for Preoperative Staging in Gastric Cancer Patients
- Non-Malignant 18F-FDG Uptake in the Thorax by Positron Emission Tomography Computed Tomography Fusion Imaging
