Cerebellar Hemorrhage due to a Direct Carotid–Cavernous Fistula after Surgery for Maxillary Cancer
- Affiliations
-
- 1Department of Neurosurgery, Hamamatsu University School of Medicine, Hamamatsu, Japan. kamio880@hotmail.com
- 2Department of Radiology, Hamamatsu University School of Medicine, Hamamatsu, Japan.
- KMID: 2365592
- DOI: http://doi.org/10.3340/jkns.2015.1206.001
Abstract
- Infratentorial cerebral hemorrhage due to a direct carotid-cavernous fistula (CCF) is very rare. To our knowledge, only four such cases have been reported. Cerebellar hemorrhage due to a direct CCF has not been reported. We describe a 63-year-old female who presented with reduced consciousness 3 days after undergoing a maxillectomy for maxillary cancer. Computed tomography showed a cerebellar hemorrhage. Magnetic resonance angiography showed a left-sided direct CCF draining into the left petrosal and cerebellar veins through the left superior petrosal sinus (SPS). Her previous surgery had sacrificed the pterygoid plexus and facial vein. Increased blood flow and reduced drainage could have led to increased venous pressure in infratentorial veins, including the petrosal and cerebellar veins. The cavernous sinus has several drainage routes, but the SPS is one of the most important routes for infratentorial venous drainage. Stenosis or absence of the posterior segment of the SPS can also result in increased pressure in the cerebellar and pontine veins. We emphasize that a direct CCF with cortical venous reflux should be precisely evaluated to determine the hemodynamic status and venous drainage from the cavernous sinus.
MeSH Terms
Figure
-
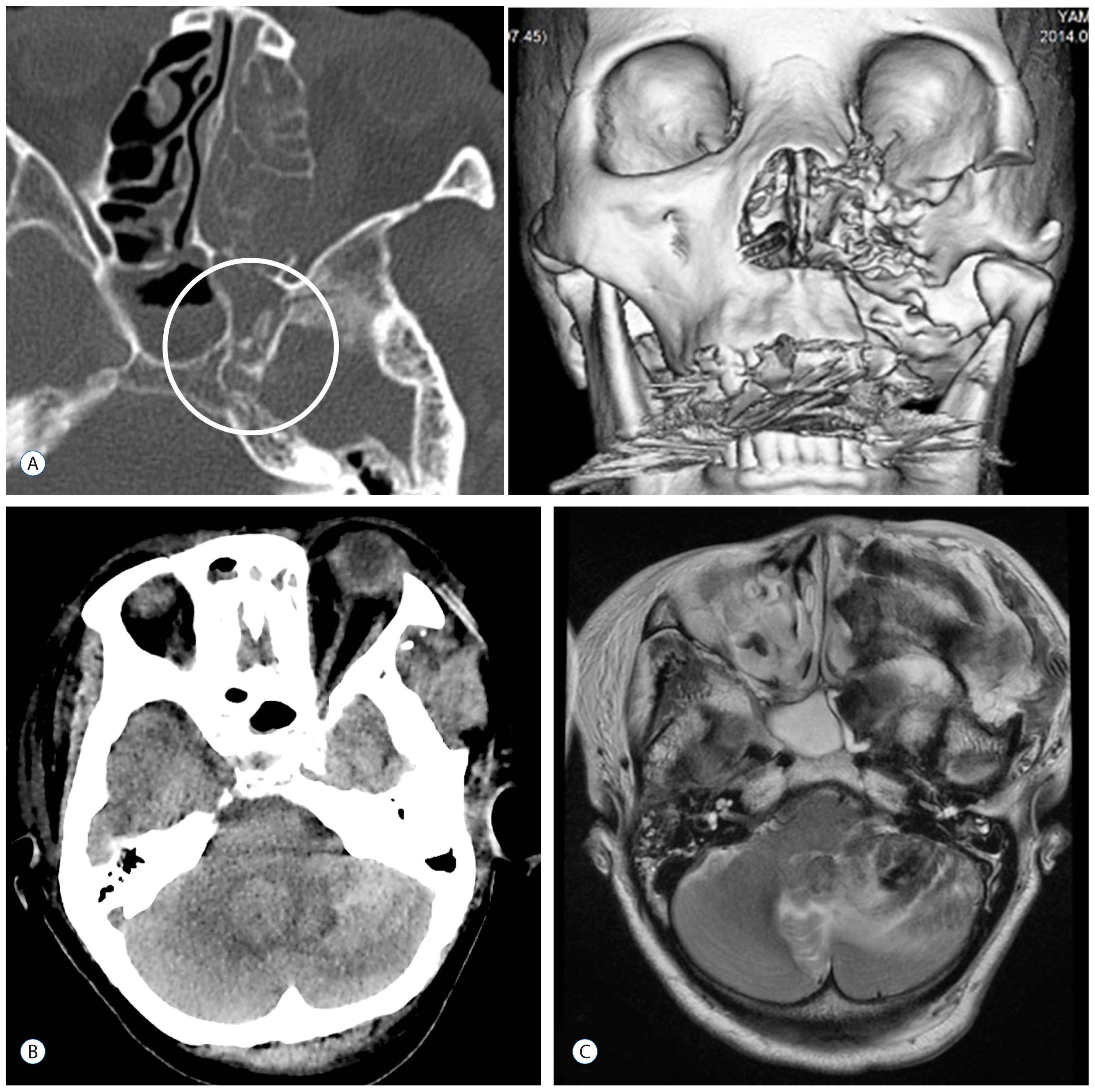
Fig. 1 CT bone image and 3D reconstruction (A) showing absence of the resected pterygoid process, and a bony spicule adjacent to the foramen lacerum (open circle). CT (B) and T2-weighted MRI (C) showed a left cerebellar hemorrhage and surrounding edema. CT: computed tomography, MRI: magnetic resonance imaging.
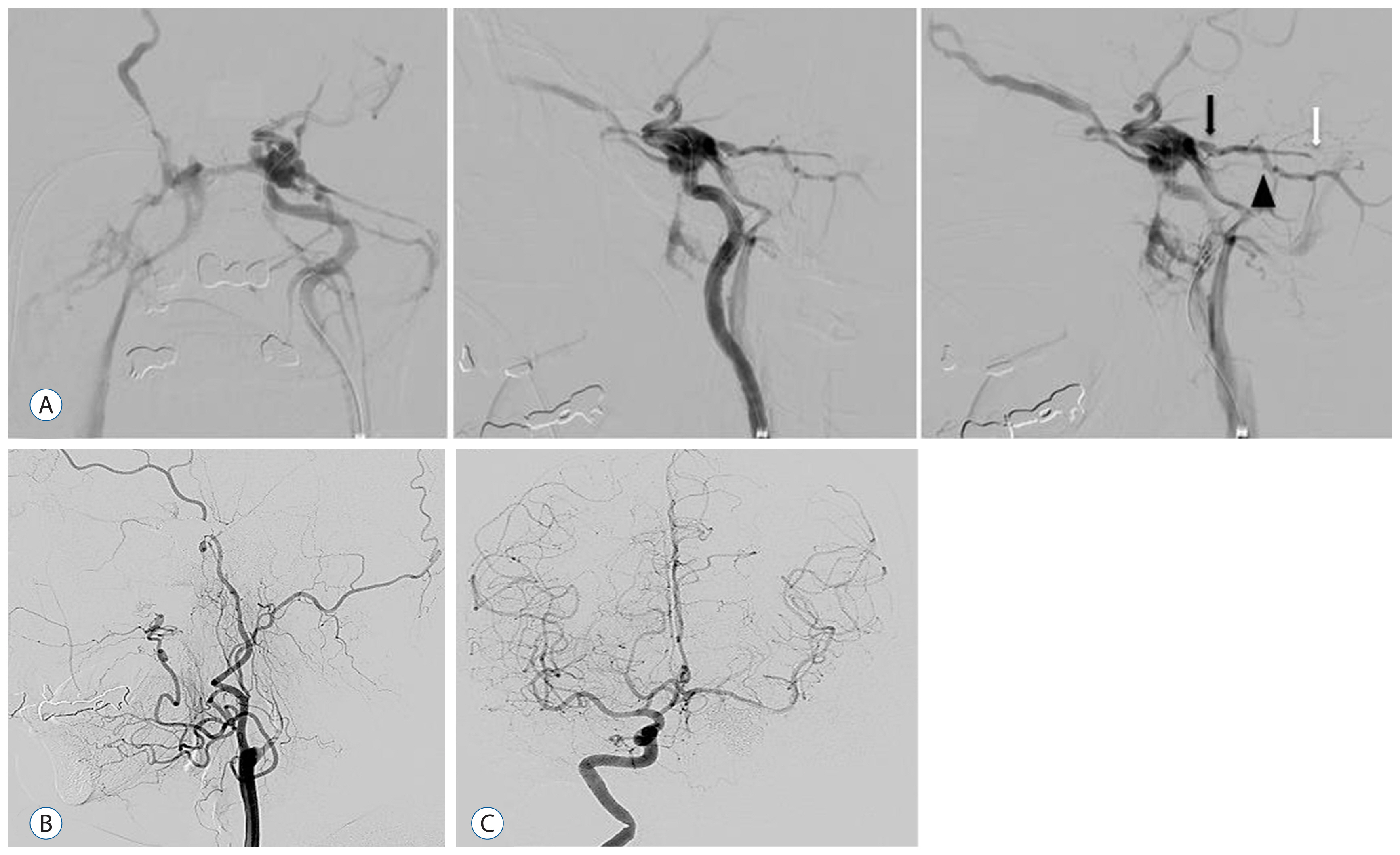
Fig. 2 The internal carotid artery angiogram (A) just before embolization, showing a high-flow direct carotid–cavernous fistula, engorgement of the proximal superior petrosal sinus (black arrow) and petrosal vein (black arrowhead), stenosis of the posterior segment of the superior petrosal sinus, and narrowing of the sigmoid sinus ostia (white arrow). B: Lateral view of the left carotid angiogram after embolization, showing disappearance of the fistula, cortical reflux, and occlusion of the internal carotid artery. C: Frontal view of the right internal carotid artery angiogram after embolization, showing left middle cerebral artery via anterior communicating artery and no visualization of the left internal carotid artery or the carotid–cavernous fistula.
Cited by 1 articles
-
Delayed intracerebral hemorrhage from a traumatic carotid-cavernous fistula associated with an enucleated orbit
Richard Bram, Nauman Chaudhry, Jason Lee Choi, Gursant Atwal
J Cerebrovasc Endovasc Neurosurg. 2021;23(3):251-259. doi: 10.7461/jcen.2021.E2020.10.006.
Reference
-
References
1. Bartlow B, Penn RD. Carotid-cavernous sinus fistula presenting as a posterior fossa mass. Case report. J Neurosurg. 42:585–588. 1975.2. d’Angelo VA, Monte V, Scialfa G, Fiumara E, Scitti G. Intracerebral venous hemorrhage in “high-risk” carotid-cavernous fistula. Surg Neurol. 30:387–390. 1983.
Article3. Hayashi K, Suyama K, Nagata I. Traumatic carotid cavernous fistula complicated with intracerebral hemorrhage: case report. Neurol Med Chir (Tokyo). 51:214–216. 2011.
Article4. Iida K, Uozumi T, Arita K, Nakahara T, Ohba S, Satoh H. Steal phenomenon in a traumatic carotid-cavernous fistula. J Trauma. 39:1015–1017. 1995.
Article5. Lewis AI, Tomsick TA, Tew JM Jr, Lawless MA. Long term results in direct carotid-cavernous fistula after treatment with detachable balloons. J Neurosurg. 84:400–404. 1996.
Article6. Moon KY, Kang SD. Spontaneous intracerebral hematoma from transient occult carotid-cavernous fistula: a case report. J Korean Med Sci. 20:166–168. 2005.
Article7. Murata H, Kubota T, Murai M, Kanno H, Fujii S, Yamamoto I. Brainstem congestion caused by direct carotid-cavernous fistula: case report. Neurol Med Chir (Tokyo). 43:255–258. 2003.
Article8. Padget DH. The development of the cranial venous system in man, from the viewpoint of comparative anatomy. Contrib Embryol. 36:79–140. 1957.9. Sattler CH. Pulsierender exophthalmus. Handbuch der Gesamten Augenheilkunde. Berlin: Springer;1920. p. 1–268.
Article10. Shimada R, Kiyosue H, Tanoue S, Mori H, Abe T. Superior petrosal sinus: hemodynamic features in normal and cavernous sinus dural arteriovenous fistulas. AJNR Am J Neuroradiol. 34:609–615. 2013.
Article11. Teng MM, Chang T, Pan DH, Chang CN, Huang CI, Guo WY, et al. Brainstem edema: an unusual complication of carotid cavernous fistula. AJNR Am J Neuroradiol. 12:139–142. 1991.12. Turner DM, Vangilder JC, Mojtahedi S, Pierson EW. Spontaneous intracerebral hematoma in carotid-cavernous fistula. Report of three cases. J Neurosurg. 59:680–686. 1983.13. Vaghi MA, Savoiardo M, Strada L. Unusual computerized tomography appearance of a carotid-cavernous fistula. Case report. J Neurosurg. 58:435–437. 1983.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Traumatic Carotid-cavernous Fistula Bringing about Intracerebral Hemorrhage
- Direct Microsurgical Repair of Traumatic Carotid-Cavernous Fistula
- Delayed Spontaneous Thrombosis of Neglected Direct Carotid-Cavernous Fistula: A Case Report
- A Case of the Carotid-Cavernous Fistula Due to the Internal Carotid Artery Injury During Endoscopic Sinus Surgery
- Carotid Cavernous Sinus Fistula with Abducens Nerve Palsy after Le Fort I Osteotomy: A Case Report
