Delayed Spontaneous Thrombosis of Neglected Direct Carotid-Cavernous Fistula: A Case Report
- Affiliations
-
- 1Department of Diagnostic and Interventional Radiology, All India Institute of Medical Sciences, Jodhpur, India
- KMID: 2503396
- DOI: http://doi.org/10.5469/neuroint.2020.00094
Abstract
- Direct carotid-cavernous fistula (CCF) refers to direct communication between the cavernous portion of the internal carotid artery (ICA) and the cavernous sinus due to rent in the ICA, most commonly secondary to trauma. These are generally high-flow fistula and rarely resolve spontaneously. We report a case of a young male who developed features of direct CCF after trauma, was denied any treatment for 4 years, and then presented with spontaneous thrombosis of the fistula and a residual large pseudoaneurysm of the cavernous segment of the right ICA, which was subsequently managed with parent vessel occlusion.
Keyword
Figure
-

Fig. 1. Magnetic resonance imaging of the brain in May 2018. The axial T2 image (A) and source images of time-of-flight magnetic resonance angiography (B) showed aneurysm dilatation of right cavernous sinus with a dilated superior ophthalmic vein (arrow). Note the prominent right inferior petrosal sinus (C, arrowhead). The imaging feature is consistent with a right-sided direct carotid-cavernous fistula. (D) shows antegrade flow within the distal right supraclinoid internal carotid artery. The axial susceptibility-weighted images (E, F) do not show any cortical venous engorgement.
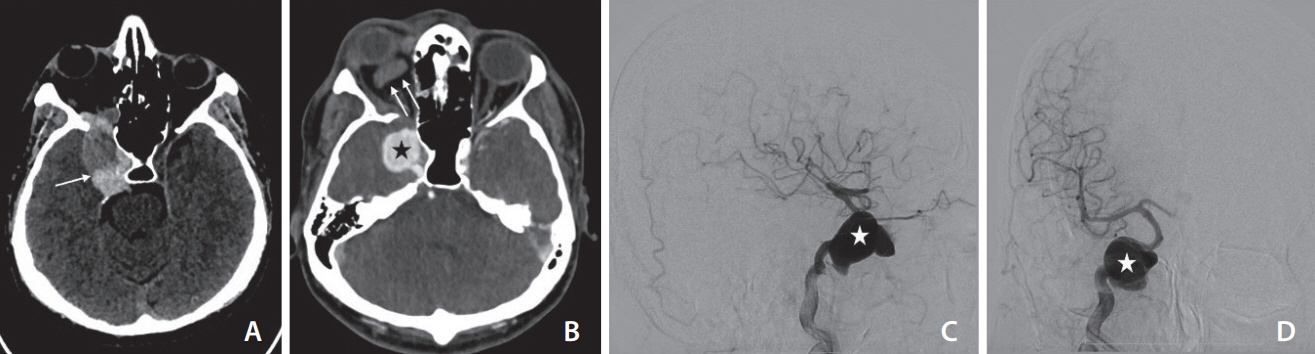
Fig. 2. The non-contrast computed tomography (CT) taken in December 2019 shows a partially thrombosed (arrow) and distended right cavernous sinus (A). The contrast-enhanced CT (B) shows thrombosis (non-opacification) of the right superior ophthalmic vein (double arrows) with a large pseudoaneurysm (asterisk) from the cavernous segment of the right internal carotid artery (ICA). The lateral (C) and antero-posterior (D) projection of the digital subtraction angiogram of the right ICA confirms the pseudoaneurysm of the right ICA (asterisk) with no opacification carotid-cavernous fistula.
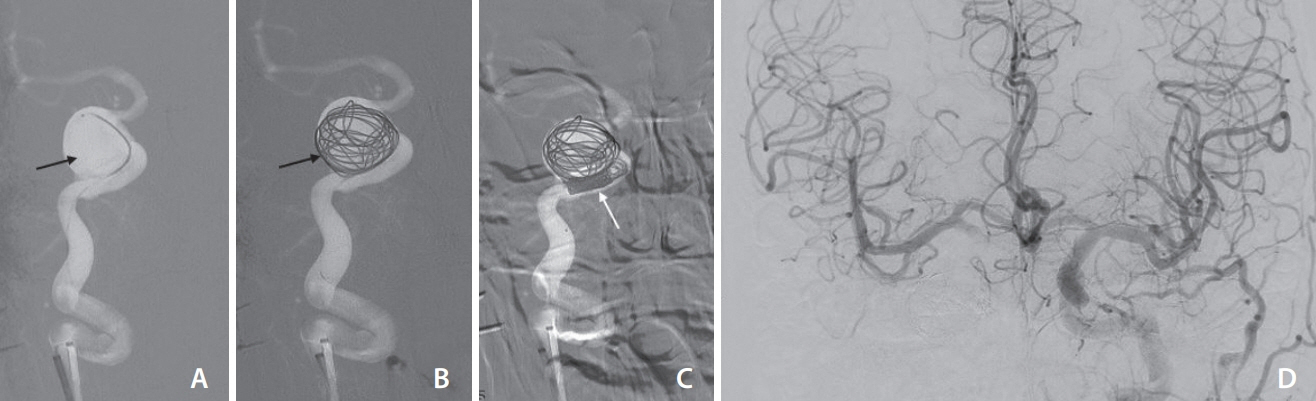
Fig. 3. The right internal carotid artery (ICA) pseudoaneurysm was managed with partial coiling of the sac (A–C), and subsequent occlusion of the petrous segment of the right ICA. The left ICA injection antero-posterior projection (D) shows good crossflow across the anterior communicating artery to opacify the right ICA circulation. There was no significant venous delay.
Reference
-
1. Iampreechakul P, Tirakotai W, Tanpun A, Wattanasen Y, Lertbusayanukul P, Siriwimonmas S. Spontaneous resolution of direct carotid-cavernous fistulas: case series and literature review. Interv Neuroradiol. 2019; 25:71–89.
Article2. Barrow DL, Spector RH, Braun IF, Landman JA, Tindall SC, Tindall GT. Classification and treatment of spontaneous carotid-cavernous sinus fistulas. J Neurosurg. 1985; 62:248–256.
Article3. Henderson AD, Miller NR. Carotid-cavernous fistula: current concepts in aetiology, investigation, and management. Eye (Lond). 2018; 32:164–172.
Article4. van Rooij WJ, Sluzewski M, Beute GN. Ruptured cavernous sinus aneurysms causing carotid cavernous fistula: incidence, clinical presentation, treatment, and outcome. AJNR Am J Neuroradiol. 2006; 27:185–189.5. Halbach VV, Hieshima GB, Higashida RT, Reicher M. Carotid cavernous fistulae: indications for urgent treatment. AJR Am J Roentgenol. 1987; 149:587–593.
Article6. Ellis JA, Goldstein H, Connolly ES Jr, Meyers PM. Carotid-cavernous fistulas. Neurosurg Focus. 2012; 32:E9.
Article7. Kai Y, Hamada J, Morioka M, Yano S, Kuratsu J. Treatment of cavernous sinus dural arteriovenous fistulae by external manual carotid compression. Neurosurgery. 2007; 60:253–257. discussion 257-258.
Article8. Nishijima M, Iwai R, Horie Y, Oka N, Takaku A. Spontaneous occlusion of traumatic carotid cavernous fistula after orbital venography. Surg Neurol. 1985; 23:489–492.
Article9. van der Drift JH, Sparling CM, van den Berg D, Magnus O. Spontaneous occlusion of a carotid-cavernous shunt. Neurology. 1967; 17:187–193.
Article10. Castillo M, Silverstein M, Hoffman JC Jr, Barrow D. Spontaneous thrombosis of a direct carotid cavernous sinus fistula: confirmation by Gd-DTPA-enhanced MR. AJNR Am J Neuroradiol. 1989; 10(5 Suppl):S75–S76.11. Alqadi M, Brunozzi D, Linninger A, Amin-Hanjani S, Charbel FT, Alaraj A. Cerebral arteriovenous malformation venous stenosis is associated with hemodynamic changes at the draining vein-venous sinus junction. Med Hypotheses. 2019; 123:86–88.
Article12. Uchino A, Takase Y, Koizumi T, Kudo S. Spontaneous thrombosis of a high-flow carotid-cavernous fistula after failed transarterial balloon occlusion. Interv Neuroradiol. 2004; 10:253–256.
Article13. Graves VB, Strother CM, Weinstein JM, Letellier M. Giant intracavernous carotid aneurysm after spontaneous thrombosis of a carotid cavernous sinus fistula. AJNR Am J Neuroradiol. 1988; 9:595–597.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Spontaneous of Traumatic Carotid Cavernous Fistula After Carotid Angiography
- Regional Cerebral Blood Flow Changes in Traumatic Carotid Cavernous Fistula During Trapping Procedure: Case Study, Preliminary Report
- Direct Microsurgical Repair of Traumatic Carotid-Cavernous Fistula
- Carotid-Cavernous Fistula Due to Giant Aneurysm in a Postpartum Woman
- Direct Surgical Approach of the Spontaneous Carotid Cavernous Fistula
