Role of Transesophageal Echocardiography in the Diagnosis of Paradoxical Low Flow, Low Gradient Severe Aortic Stenosis
- Affiliations
-
- 1Division of Cardiovascular Diseases, Department of Internal Medicine, Mayo Clinic, Scottsdale, AZ, USA. Chaliki.Hari@mayo.edu
- KMID: 2365286
- DOI: http://doi.org/10.4070/kcj.2016.0126
Abstract
- BACKGROUND AND OBJECTIVES
Prior studies indicate that up to 35% of cases of severe aortic stenosis (AS) have paradoxical low flow, low gradient despite preserved left ventricular ejection fraction (LVEF). However, error in left ventricular outflow tract (LVOT) diameter may lead to misclassification. Herein, we determined whether measurement of LVOT diameter by transesophageal echocardiography (TEE) results in reclassification of cases to non-severe AS.
SUBJECTS AND METHODS
Patients with severe AS with aortic valve area (AVA) <1 cm2 by transthoracic echocardiography (TTE) within 6 months were studied. Paradoxical low flow, low gradient was defined as mean Doppler gradient (MG) <40 mm Hg and stroke volume index (SVI) ≤35 mL/m². Preserved LVEF was defined as ≥0.50.
RESULTS
Among 108 patients, 12 (15%) had paradoxical low flow, low gradient severe AS despite preserved LVEF based on TTE measurement. When LVOT diameter by TEE in 2D was used, only 5 (6.3%) patients had low flow, low gradient severe AS (p<0.001). Coefficients of variability for intraobserver and interobserver measurement of LVOT were <10%. However, the limits of agreement between TTE and TEE measurement of LVOT ranged from 0.43 cm (95% confidence interval [CI]: 0.36 to 0.5) to -0.31 cm (95% CI: -0.38 to -0.23).
CONCLUSION
TEE measured LVOT diameter may result in reclassification to moderate AS in some patients due to low prevalence of true paradoxical low flow, low gradient (PLFLG) severe AS.
Keyword
MeSH Terms
Figure
-
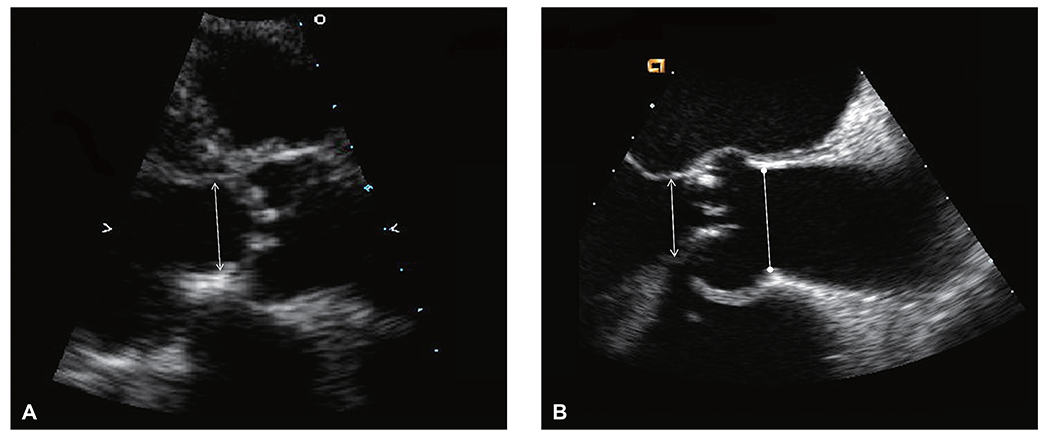
Fig. 1 Measurement of left ventricular outflow tract diameter by transthoracic and transesophageal echocardiography. (A) On transthoracic echocardiography, left ventricular outflow tract diameter (arrow) is measured in mid-systole from inner edge to inner edge just below insertion of the aortic valve leaflets. (B) On transesophageal echocardiography, left ventricular outflow tract diameter (arrow) is measured in mid-systole from inner edge to inner edge. Sinotubular junction diameter (arrow with rounded edges) is also shown.

Fig. 2 TEE reclassification of patients with severe AS and normal LV ejection fraction. By transesophageal echocardiography, a significant number of patients with severe aortic stenosis are reclassified, particularly in the low flow and low flow, low gradient severe aortic stenosis groups. TTE: transthoracic echocardiography, AS: aortic stenosis, LV: left ventricle, TEE: transesophageal echocardiography.
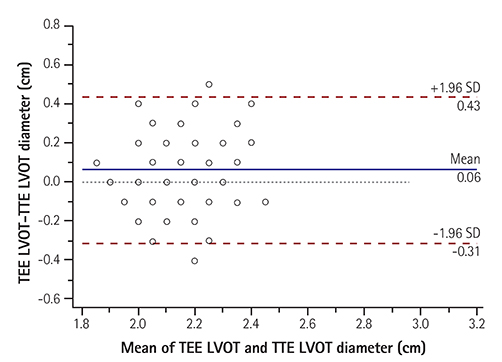
Fig. 3 Bland-Altman plot demonstrating trend of underestimation by TTE. The wide limits of agreement between transthoracic and transesophageal echocardiography measurement likely explains reclassification of patients on the basis of left ventricular outflow tract diameter measurement. TEE: transesophageal echocardiography, LVOT: left ventricular outflow tract, TTE: transthoracic echocardiogram, SD: standard deviation.
Cited by 1 articles
-
Natural History Data in Symptomatic Severe Aortic Stenosis Alerts Cardiologists to the Dangers of No Action
Hyun-Jung Lee, Hyung-Kwan Kim
Korean Circ J. 2019;49(2):170-172. doi: 10.4070/kcj.2018.0344.
Reference
-
1. Nkomo VT, Gardin JM, Skelton TN, Gottdiener JS, Scott CG, Enriquez-Sarano M. Burden of valvular heart diseases: a population-based study. Lancet. 2006; 368:1005–1011.2. Baumgartner H, Hung J, Bermejo J, et al. Echocardiographic assessment of valve stenosis: EAE/ASE recommendations for clinical practice. J Am Soc Echocardiogr. 2009; 22:1–23. quiz 101-2.3. Nishimura RA, Otto CM, Bonow RO, et al. 2014 AHA/ACC Guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014; 129:e521–e643.4. Hachicha Z, Dumesnil JG, Bogaty P, Pibarot P. Paradoxical low-flow, low-gradient severe aortic stenosis despite preserved ejection fraction is associated with higher afterload and reduced survival. Circulation. 2007; 115:2856–2864.5. Pibarot P, Dumesnil JG. Assessment of aortic stenosis severity: when the gradient does not fit with the valve area. Heart. 2010; 96:1431–1433.6. Zoghbi WA, Farmer KL, Soto JG, Nelson JG, Quinones MA. Accurate noninvasive quantification of stenotic aortic valve area by Doppler echocardiography. Circulation. 1986; 73:452–459.7. Garcia D, Pibarot P, Dumesnil JG, Sakr F, Durand LG. Assessment of aortic valve stenosis severity: A new index based on the energy loss concept. Circulation. 2000; 101:765–771.8. Hachicha Z, Dumesnil JG, Pibarot P. Usefulness of the valvuloarterial impedance to predict adverse outcome in asymptomatic aortic stenosis. J Am Coll Cardiol. 2009; 54:1003–1011.9. Altiok E, Koos R, Schroder J, et al. Comparison of two-dimensional and three-dimensional imaging techniques for measurement of aortic annulus diameters before transcatheter aortic valve implantation. Heart. 2011; 97:1578–1584.10. Messika-Zeitoun D, Serfaty JM, Brochet E, et al. Multimodal assessment of the aortic annulus diameter: implications for transcatheter aortic valve implantation. J Am Coll Cardiol. 2010; 55:186–194.11. Utsunomiya H, Yamamoto H, Horiguchi J, et al. Underestimation of aortic valve area in calcified aortic valve disease: effects of left ventricular outflow tract ellipticity. Int J Cardiol. 2012; 157:347–353.12. Kempfert J, Van Linden A, Lehmkuhl L, et al. Aortic annulus sizing: echocardiographic versus computed tomography derived measurements in comparison with direct surgical sizing. Eur J Cardiothorac Surg. 2012; 42:627–633.13. Shiran A, Adawi S, Ganaeem M, Asmer E. Accuracy and reproducibility of left ventricular outflow tract diameter measurement using transthoracic when compared with transesophageal echocardiography in systole and diastole. Eur J Echocardiogr. 2009; 10:319–324.14. Pibarot P, Garcia D, Dumesnil JG. Energy loss index in aortic stenosis: from fluid mechanics concept to clinical application. Circulation. 2013; 127:1101–1104.15. Ng AC, Delgado V, van der Kley F, et al. Comparison of aortic root dimensions and geometries before and after transcatheter aortic valve implantation by 2- and 3-dimensional transesophageal echocardiography and multislice computed tomography. Circ Cardiovasc Imaging. 2010; 3:94–102.16. Clavel MA, Rodes-Cabau J, Dumont E, et al. Validation and characterization of transcatheter aortic valve effective orifice area measured by Doppler echocardiography. JACC Cardiovasc Imaging. 2011; 4:1053–1062.17. Pibarot P, Dumesnil JG. Low-flow, low-gradient aortic stenosis with normal and depressed left ventricular ejection fraction. J Am Coll Cardiol. 2012; 60:1845–1853.18. Jander N, Minners J, Holme I, et al. Outcome of patients with low-gradient “severe” aortic stenosis and preserved ejection fraction. Circulation. 2011; 123:887–895.19. Tribouilloy C, Rusinaru D, Marechaux S, et al. Low-gradient, low-flow severe aortic stenosis with preserved left ventricular ejection fraction: characteristics, outcome, and implications for surgery. J Am Coll Cardiol. 2015; 65:55–66.20. Kim KS, Maxted W, Nanda NC, et al. Comparison of multiplane and biplane transesophageal echocardiography in the assessment of aortic stenosis. Am J Cardiol. 1997; 79:436–441.21. Malyar NM, Schlosser T, Barkhausen J, et al. Assessment of aortic valve area in aortic stenosis using cardiac magnetic resonance tomography: comparison with echocardiography. Cardiology. 2008; 109:126–134.22. Reant P, Lederlin M, Lafitte S, et al. Absolute assessment of aortic valve stenosis by planimetry using cardiovascular magnetic resonance imaging: comparison with transesophageal echocardiography, transthoracic echocardiography, and cardiac catheterisation. Eur J Radiol. 2006; 59:276–283.23. Khaw AV, von Bardeleben RS, Strasser C, et al. Direct measurement of left ventricular outflow tract by transthoracic real-time 3D-echocardiography increases accuracy in assessment of aortic valve stenosis. Int J Cardiol. 2009; 136:64–71.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Paradoxical Low-Flow, Low-Gradient Aortic Stenosis–a Tough Nut to Crack in Echocardiographic Diagnosis
- Multiplane Transesophageal Echocardiographic Findings of Two Cases of Discrete Subvalvular Aortic Stenosis
- Doppler Echocardiographic Findings in the Elderly with Aortic Stenosis
- Left Atrial Dissection by Aorto-Left Atrial Fistula after Aortic Valve Replacement: A case report
- Exercise Echocardiography in Asymptomatic Patients with Severe Aortic Stenosis and Preserved Left Ventricular Ejection Fraction
