Doppler Echocardiographic Findings in the Elderly with Aortic Stenosis
- Affiliations
-
- 1Department of Internal Medicine, College of Medicine, Pusan National University, Pusan, Korea.
- KMID: 2410457
- DOI: http://doi.org/10.4250/jkse.1994.2.1.32
Abstract
- BACKGROUND
Because of rarity of study on aortic stenosis in the elderly which has progressively increased the clinical significance, we have performed this study to assess the degree and the clinical significance of aortic stenosis in the elderly. METHOD: According to the clinical features and echocardiographic findings, we have analyzed the trans-aortic peak pressure gradient, trans-aortic mean pressure gradient, left ventricular outflow tract(LVOT)/trans-aortic peak velocity ratio and aortic valve area from 3889 consecutive the elderly above the age of 60 or older(mean age 68, male 1953, female 1936) using Doppler echocardiography prospectively. RESULT: We have observed 162 cases of aortic stenosis in the elderly and among this, 16 cases were bicuspid aortic stenosis. The criteriae of hemodynamically significant aortic stenosis in the elderly using Doppler echocardiography and their frequencies were 23.4% as trans-aortic peak pressure gradient 45mmHg or more, 22.2% as trans-aortic mean pressure gradient 25mmHg or more, 26.5% as LVOT/trans-aortic peak velocity ratio 0.32 or less and 26.5% as aortic valve area 1.0cm2 or less.
CONCLUSION
In the current study, we have found that trans-aortic peak pressure gradient, trans-aortic mean pressure gradient, LVOT/trans-aortic peak veolcity ratio and aortic valve area using Doppler echocardiography were useful and adjuvant in diagnosing and evaluating the aortic stenosis in the elderly.
MeSH Terms
Figure
-

Fig. 1. Bar graph of distribution of aortic peak pressure gradient.
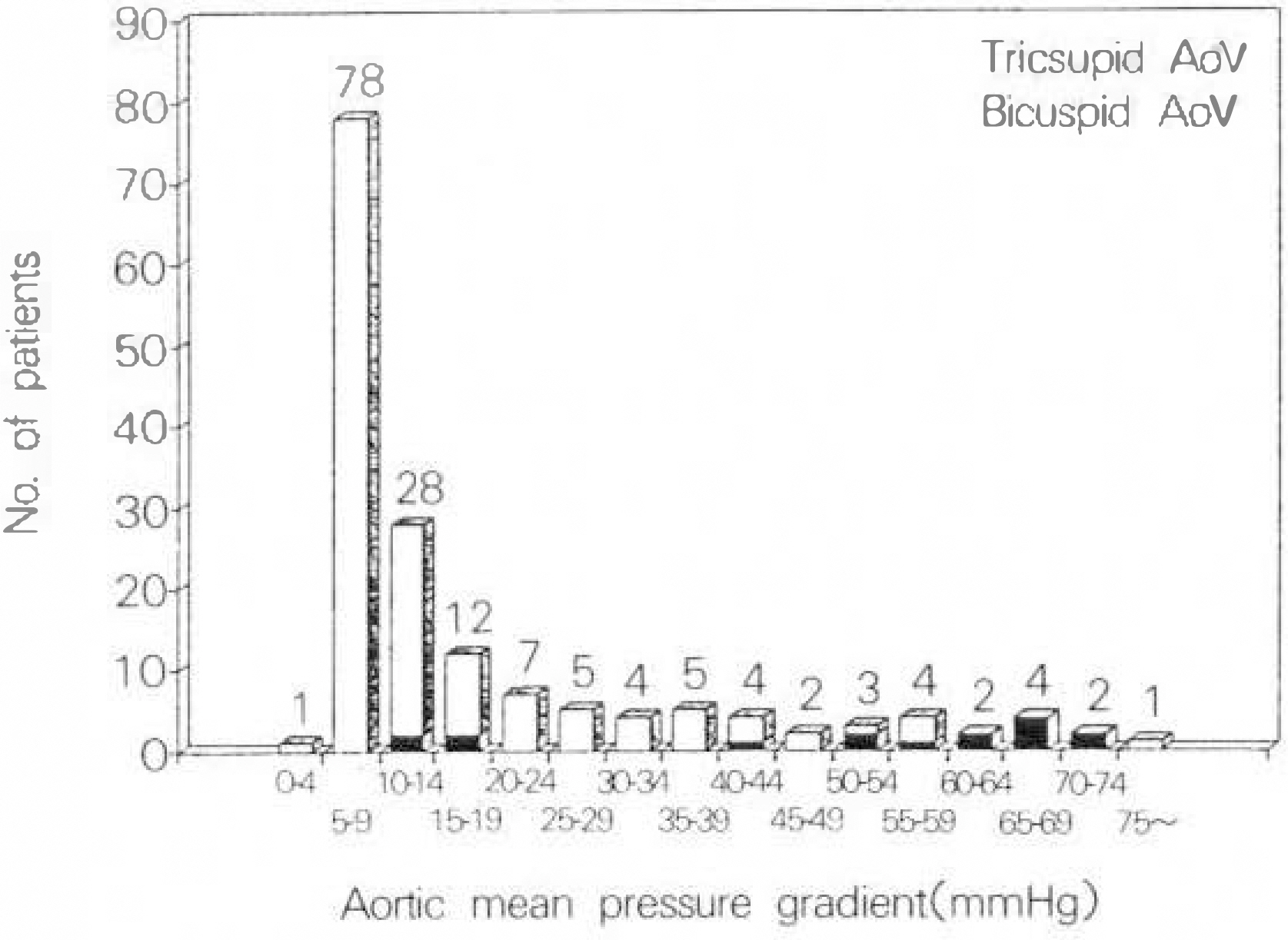
Fig. 2. Bar graph of distribution of aortic mean pressure gradient.
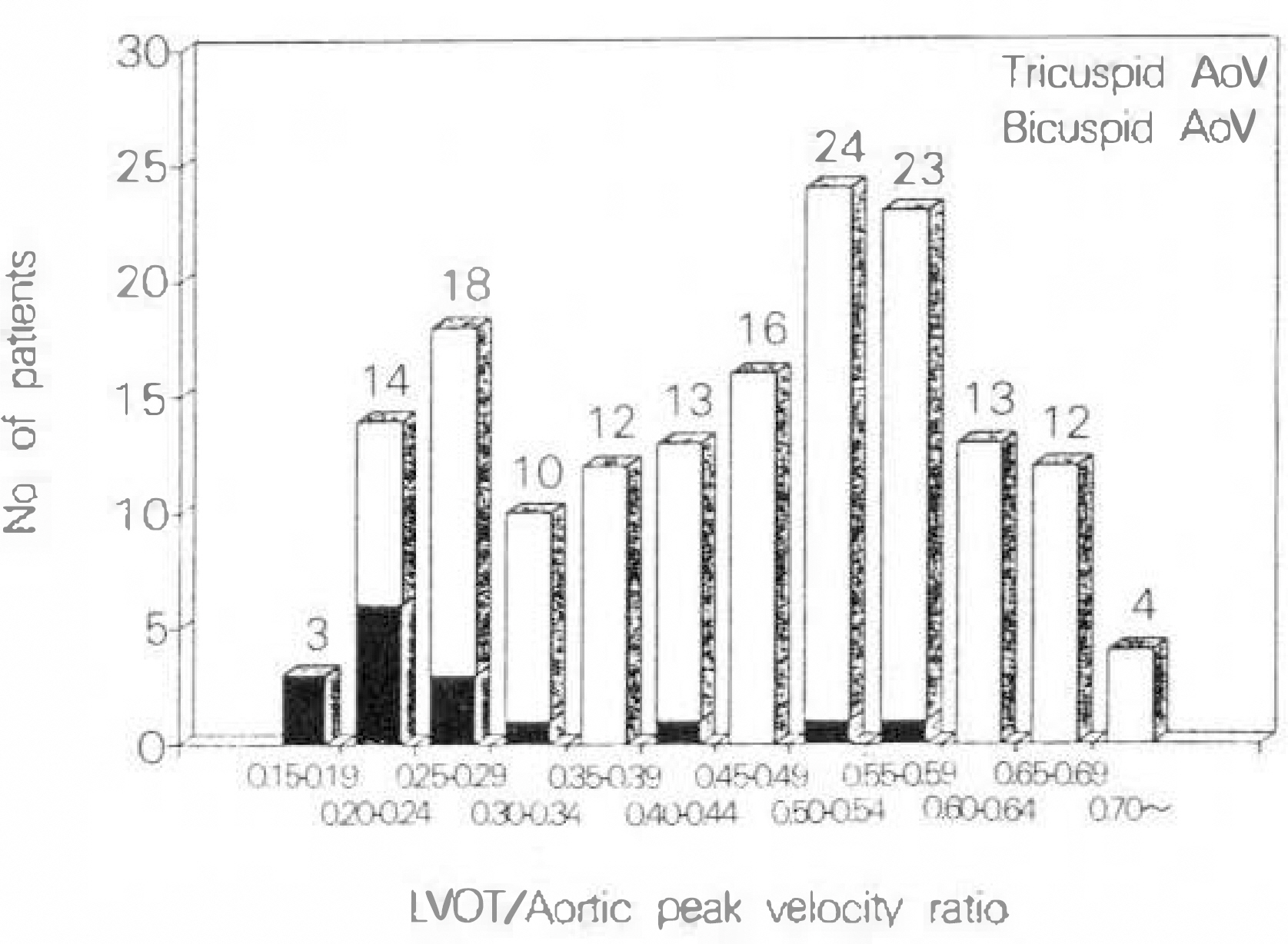
Fig. 3. Bar graph of distribution of left ventricular outflow tract(LVOT)/aortic peak velocity ratio.
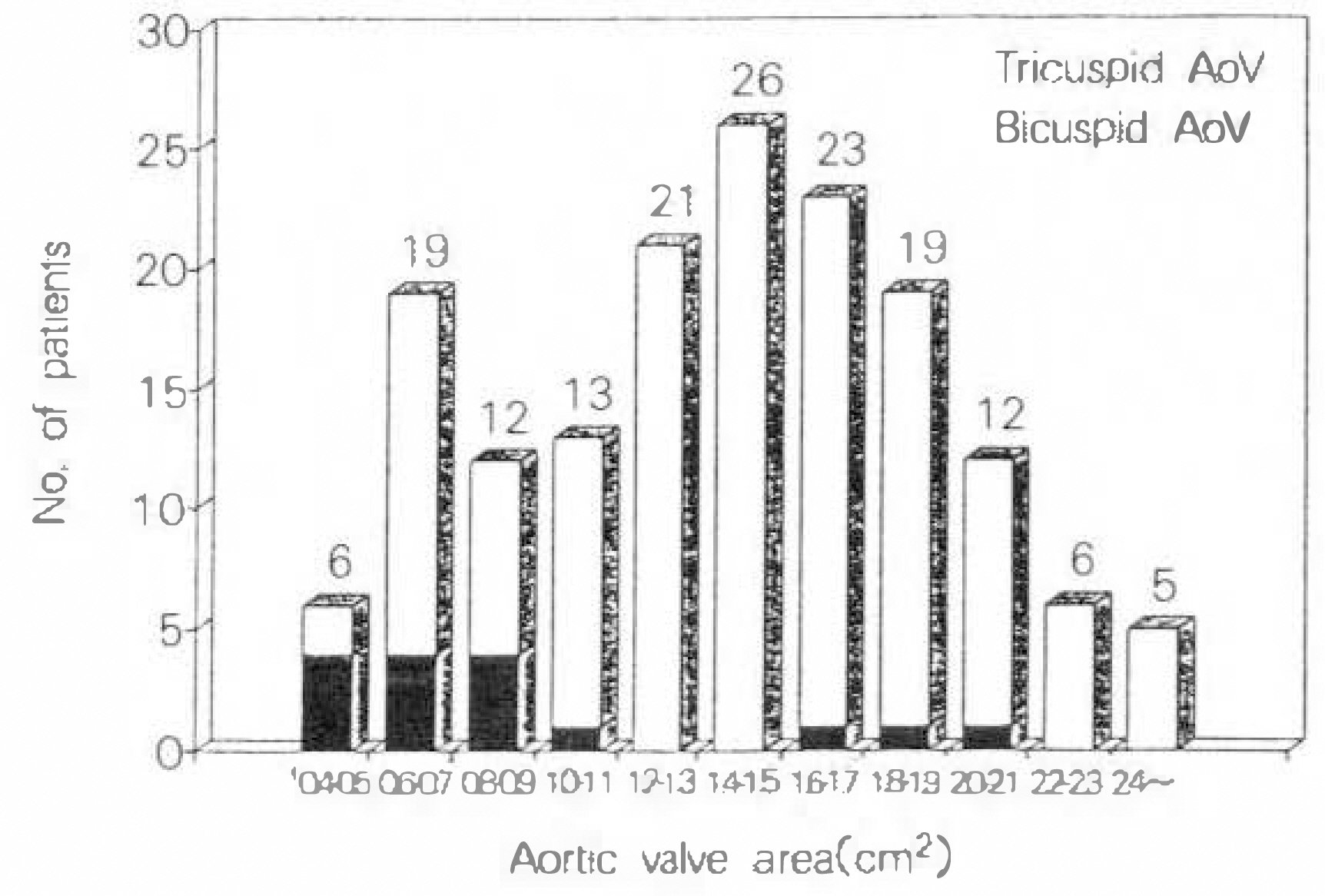
Fig. 4. Bar graph of distribution of aortic valve area.
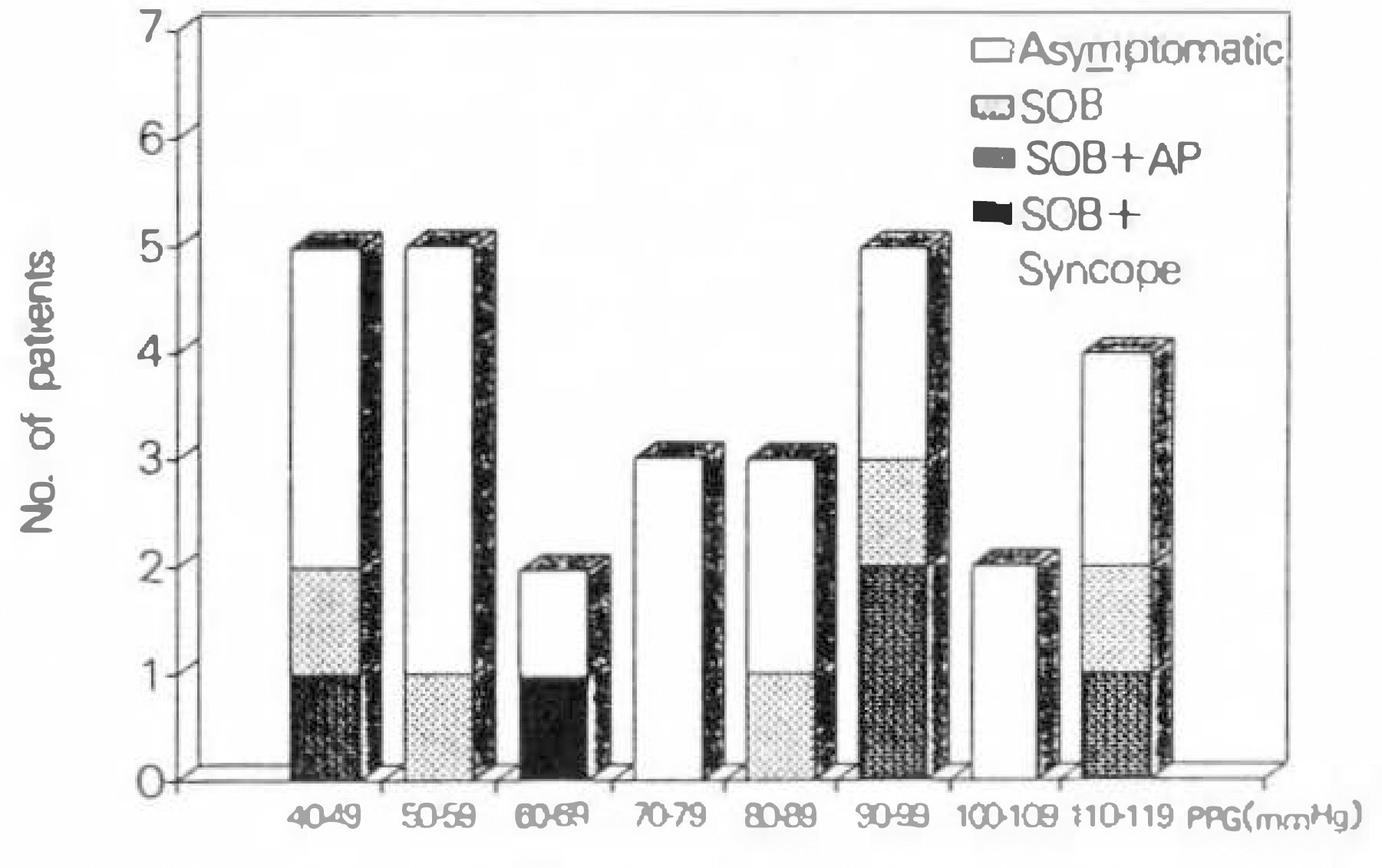
Fig. 5. Bar graph of distribution of aortic peak pressure gradient(PPG) in 29 normotensives with left ventricular hypertrophy.
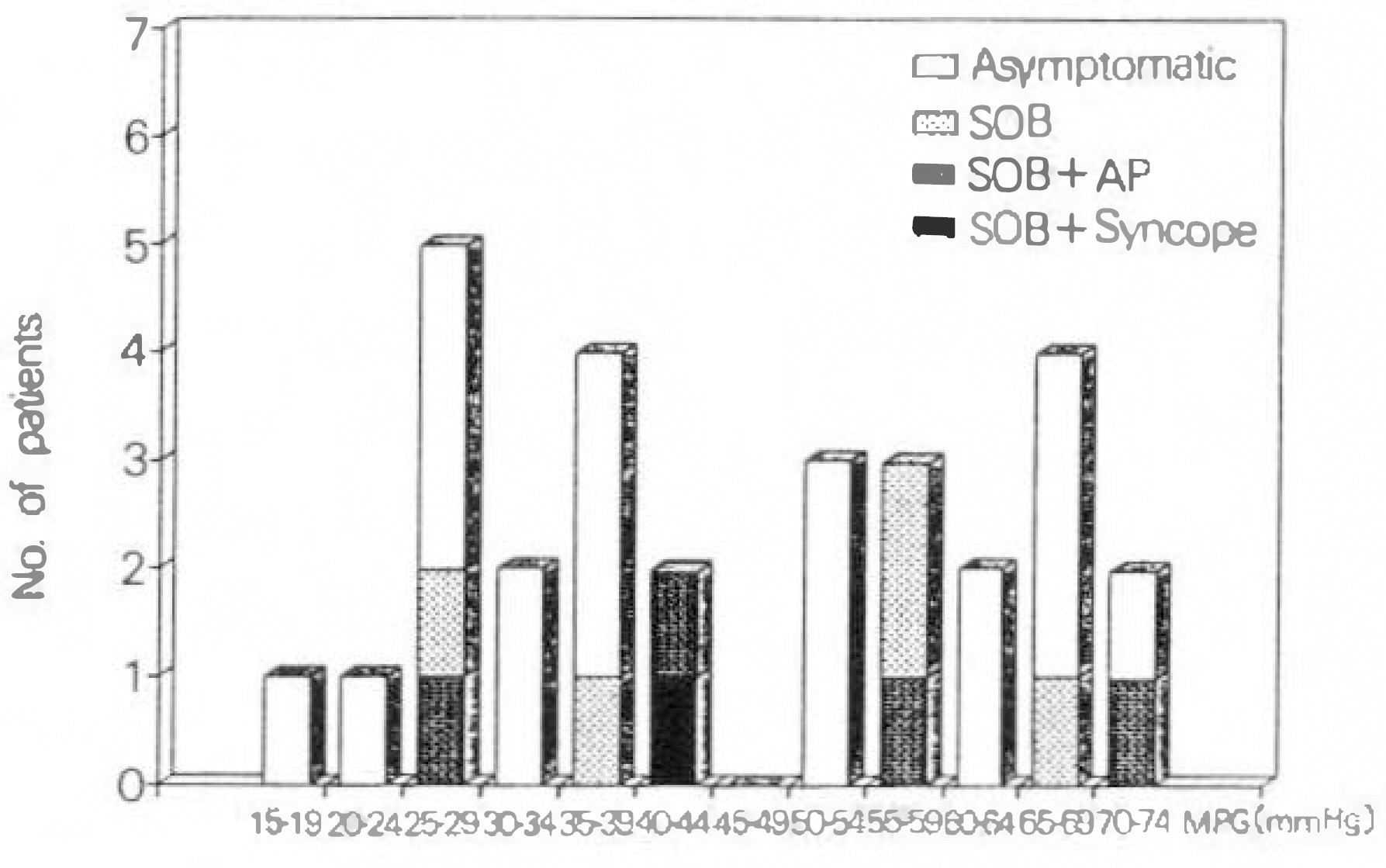
Fig. 6. Bar graph of distribution of aortic mean pressure gradient(MPG) in 29 normotensives with left ventricular hypertrophy.
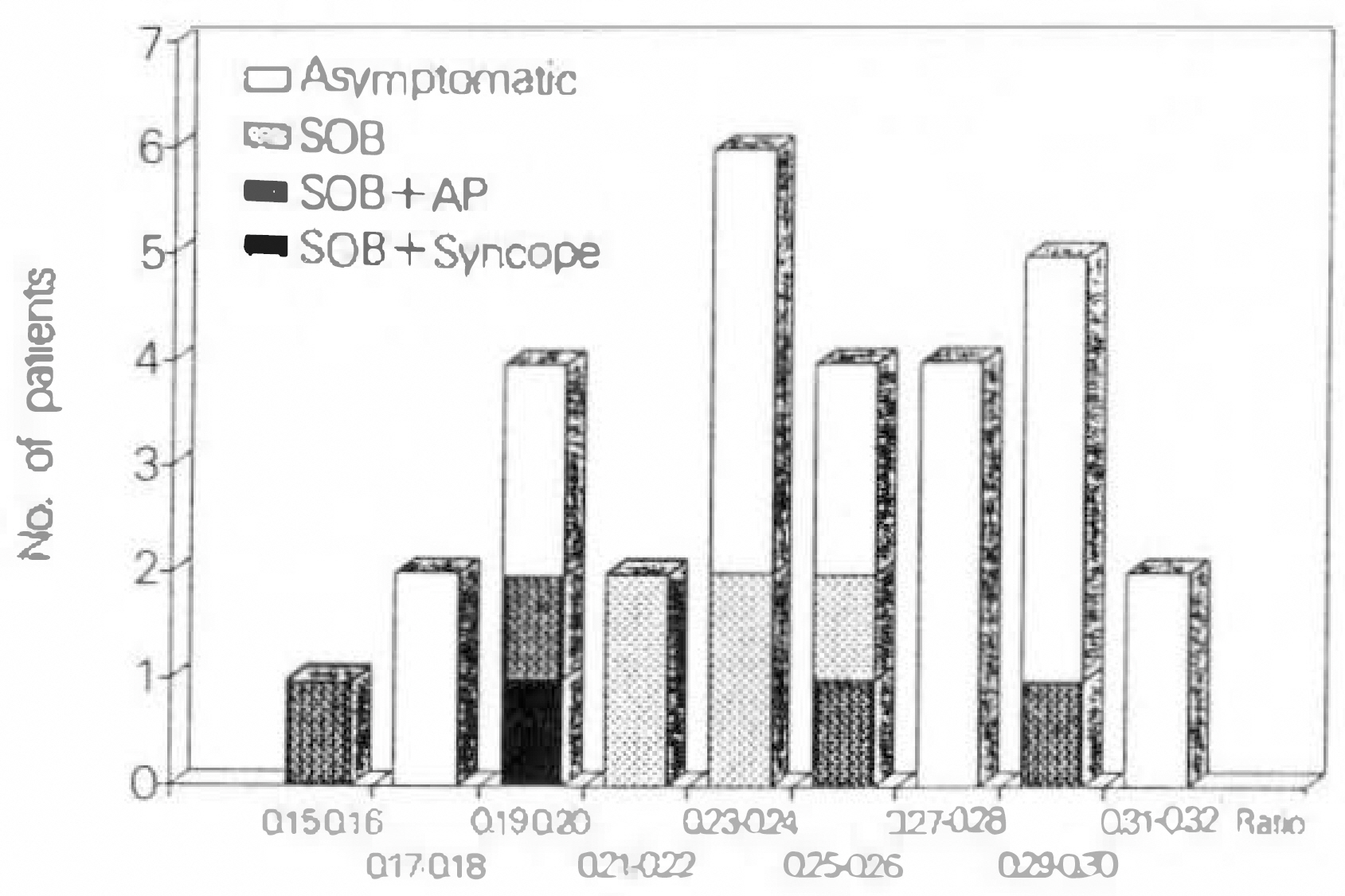
Fig. 7. Bar graph of distribution of left ventricular outflow tract(LVOT)/aortic peak velocity ratio in 29 normotensives with left ventricular hypertrophy.

Fig. 8. Bar graphy of distribution of aortic valve area (AVA) in 29 normotensives with left ventricular hypertophy.
Reference
-
References
1). Galan A, Zoghbi WA, Quinones MA. Determination of severity of valvular aortic stenosis by Doppler echocardiography and relation of findings to clinical outcome and agreement with hemodynamic measurements determined at cardiac catheterization. Am J Cardiol. 67:1007–1012. 1991.
Article2). Pollikka PA, Nishimura RA, Bailey KR, Tajik AJ. The natural history of adults with asymptomatic, hemodynamically significant aortic stenosis. J Am Coll Cardiol. 15:1012–1017. 1990.3). Brogan WC, Grayburn PA, Lange RA, Hillis LD. Prognosis after valve replacement in patients with severe aortic stenosis and a low transvalvular pressure gradient. J Am Coll Cardiol. 21:1657–1660. 1993.
Article4). Olsson M, Granstrom L, Lindblom D, Rosenqvist M, Ryden L. Aortic valve replacement in octogenarians with aortic stenosis. J Am Coll Cardiol. 20:1512–1516. 1992.5). Carroll JD, Carroll EP, Feldman T, Ward DM, Lang RM, McGaughey D, Karp RB. Sex-associated differences in left ventricular function in aortic stenosis of the elderly. Circulation. 86:1099–1107. 1992.
Article6). 신영우. 무중상 노인에서 대동맥판 비후의 빈도 및 의미. 순환기. 23:75–81. 1993.7). Sahn DJ, DeMaria A, Kisslo J. Weyman A- The committee on M-mode standardization of the american society of echocardiography: Recommendations regarding quantitation in M-mode echocardiography. Circulation. 58:1072–1083. 1978.8). Henry WL, DeMaria A, Gramiak R, King DL, Kisslo JA, Popp RL, Sahn DJ, Schiller NB, Tajik A, Teichholz LE, Weyman AE. Report of the american society of echocardiography committee on nomenclature and standards in two dimensional echocardiography. Circulation. 62:212–217. 1980.9). Skjaerpe T, Hegrenaes L, Hatle L. Noninvasive estimation of valve area in patients with aortic stenosis by Doppler ultrasound and two-dimensional echocardiography. Circulation. 72:810–818. 1985.
Article10). Yeager M, Yock PG, Popp RL. Comparison of Doppler-derived gradient to that determined at cardiac catheterization in adults with aortic stenosis: Implications for management. Am J Cardiol. 57:644–648. 1986.11). Valdes-Cruz LM, Yoganathan AP, Tamura T, Tomizuka F, Woo Y-R, Sahn DJ. Studies in vitro of the relationship between ultrasound and laser Doppler velocimetry and applicability of the simplified Bernoulli relationship. Circulation. 73:300–308. 1986.12). Berger M, Hecht SR. Doppler echocardiographic assessment of aortic stenosis using the peak velocity ratio. Am J Cardiol. 70:536–537. 1992.
Article13). Burwash IG, Thomas DD, Sadahiro M, Pearlman AS, Verrier ED, Thomas R, Kraft CD, Otto CM. Dependence of Gorlin formula and continuity equation valve area on transvalvular volume flow rate in valvular aortic stenosis. Circulation. 89:827–835. 1994.14). Aronow WS, Kronzon I. Correlation of prevalence and severity of valvular aortic stenosis determined by continuous-wave Doppler echocardiography with physical signs of aortic stenosis in patients aged 62 to 100 years with aortic systolic ejection murmurs. Am J Cardiol. 60:399–401. 1987.
Article15). Aronow WS, Kronzon I. Prevalence and severity of valvular aortic stenosis determined by Doppler echocardiography and its association with echocardiographic and electrocardiographic left ventricular hypertrophy and physical signs of aortic stenosis in elderly patients. Am J Cardiol. 67:776–777. 1991.
Article16). Isner JM, Chokshi SK, DeFranco A, Braimen J, Slovenkai GA. Contrasting histoarchitecture of calcified leaflets from stenotic bicuspid versus stenotic tricuspid aortic valves. J Am Coll Cardiol. 15:1104–1108. 1990.
Article17). Davies SW, Gershlick AH, Balcon R. Progression of valvular aortic stenosis: a long-term retrospective study. Eu Heart J. 12:10–14. 1991.18). Roger VL, Tajik AJ, Bailey KR, Oh JK, Taylor CL, Seward JB. Progression of aortic stenosis in adults: New appraisal using Doppler echocardiography. Am Heart J. 119:331–338. 1990.19). Margonato A, Cianflone D, Carlino M, Conversano A, Nitti C, Chierchia S. Frequence and significance of aortic valve thickening in older asymptomatic patients and its relation to aortic regurgitation. Am J Cardiol. 64:1061–1062. 1989.
Article20). Faggiano P, Ghizzoni G, Sorgato A, Sabatini T, Simoncelli U, Gardini A, Rusoni C. Rate of progression of valvular aortic stenosis in adults. Am J Cardiol. 70:229–233. 1992.
Article21). Warth DC, Stewart WJ, Block PC, Weyman AE. A new method to calculate aortic valve area without left heart catheterization. Circulation. 70:978–983. 1984.
Article22). Geibel A, Gornandt L, Kasper W, Bubenheimer P. Reproducibility of Doppler echocardiographic quantification of aortic and mitral valve stenosis: Comparison between two echocardiography centers. Am J Cardiol. 67:1013–1021. 1991.23). Shah P, Graham BM. Management of aortic stenosis: Is cardiac catheterization necessary ? Am J Cardiol. 67:1031–1032. 1991.24). Otto CM, Nishimura RA, Davis KB, Kisslo KB, Bashore TM. Doppler echocardiographic findings in adults with severe symptomatic valvular aortic stenosis. Am J Cardiol. 68:1477–1484. 1991.
Article25). Agatston AS, Chengot M, Rao A, Hildner F, Samet P. Doppler diagnosis of valvular aortic stenosis in patients over 60 years of age. Am J Cardiol. 56:106–109. 1985.
Article26). Lindroos M, Kupari M, Heikkila J, Tilvis R. Prevalence of aortic valve abnormalities in the elderly: An echocardiographic study of a random population sample. J Am Coll Cardiol. 21:1220–1225. 1993.
Article27). Smith MD, Dawson PL, Elion JL, Wisenbaugh T, Kwan OL, Handshoe S, DeMaria AN. Systematic correlation of continuous-wave Doppler and hemodynamic measurements in patients with aortic stenosis. Am Heart J. 111:245–252. 1986.
Article28). Dumesnil JG, Yoganathan AP. Theoretical and practical differences between the Gorlin formula and the continuity equation for calculating aortic and mitral valve areas. Am J Cardiol. 67:1268–1272. 1991.
Article29). Cannon JD, Zile MR, Crawford FA, Carabello BA. Aortic valve resistance as an adjunct to the Gorlin formula in assessing to the seventy of aortic stenosis in symptomatic patients. J Am Coll Cardiol. 20:1517–1523. 1992.30). Ford LE, Feldman T, Carrol JD. Valve resistance. Circulation. 89:893–895. 1994.
Article31). Hoffmann R, Flachskampf FA, Hanrath P. Planimetry of orifice area in aortic stenosis using multiplane transesophageal echocardiography. J Am Coll Cardiol. 22:529–534. 1993.32). Beppu S, Suzuki S, Matsuda H, Ohmori F, Nagata S, Miyatake K. Rapidity of progression of aortic stenosis in patients with congenital bicuspid aortic valves. Am J Cardiol. 71:322–327. 1993.
Article33). Roberts WC, Perloff JK, Costantino T. Severe valvular aortic stenosis in patients over 65 years of age. Am J Cardiol. 27:497–506. 1971.
Article34). Nylander E, Ekman I, Marklund T, Sinnerstad B, Karlsson E, Wranne B. Severe aortic stenosis in elderly patients. Br Heart J. 55:480–487. 1986.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Noninvasive Evaluation of Rheumatic Tricuspid Stenosis with Doppler and 2 Dimensional Echocardiography
- Value of Pulsed Doppler Echocardiography in the Diagnosis of Aortic Regurgitation
- Systolic Pressure Gradients in Aortic Valve Stenosis by Continuous Wave Doppler Echocardiography
- Assessment of Mitral Stenosis by Doppler Echocardiography: Influence of Atrial Fibrillation of Doppler Pressure Half-Time
- Frequency and significance of aortic valve thickening in the asymptomatic elderly
