J Clin Neurol.
2016 Jan;12(1):75-78. 10.3988/jcn.2016.12.1.75.
Dermatological Manifestations of Postural Tachycardia Syndrome Are Common and Diverse
- Affiliations
-
- 1Boston University School of Medicine, Boston, MA, USA. hhuang@bu.edu
- 2Department of Neurology, Boston University Medical Center, Boston, MA, USA.
- KMID: 2364922
- DOI: http://doi.org/10.3988/jcn.2016.12.1.75
Abstract
- BACKGROUND AND PURPOSE
Postural tachycardia syndrome (POTS) is a syndrome of orthostatic intolerance in the setting of excessive tachycardia with orthostatic challenge, and these symptoms are relieved when recumbent. Apart from symptoms of orthostatic intolerance, there are many other comorbid conditions such as chronic headache, fibromyalgia, gastrointestinal disorders, and sleep disturbances. Dermatological manifestations of POTS are also common and range widely from livedo reticularis to Raynaud's phenomenon.
METHODS
Questionnaires were distributed to 26 patients with POTS who presented to the neurology clinic. They were asked to report on various characteristics of dermatological symptoms, with their answers recorded on a Likert rating scale. Symptoms were considered positive if patients answered with "strongly agree" or "agree", and negative if they answered with "neutral", "strongly disagree", or "disagree".
RESULTS
The most commonly reported symptom was rash (77%). Raynaud's phenomenon was reported by over half of the patients, and about a quarter of patients reported livedo reticularis. The rash was most commonly found on the arms, legs, and trunk. Some patients reported that the rash could spread, and was likely to be pruritic or painful. Very few reported worsening of symptoms on standing.
CONCLUSIONS
The results suggest that dermatological manifestations in POTS vary but are highly prevalent, and are therefore of important diagnostic and therapeutic significance for physicians and patients alike to gain a better understanding thereof. Further research exploring the underlying pathophysiology, incidence, and treatment strategies is necessary.
Keyword
MeSH Terms
Figure
-
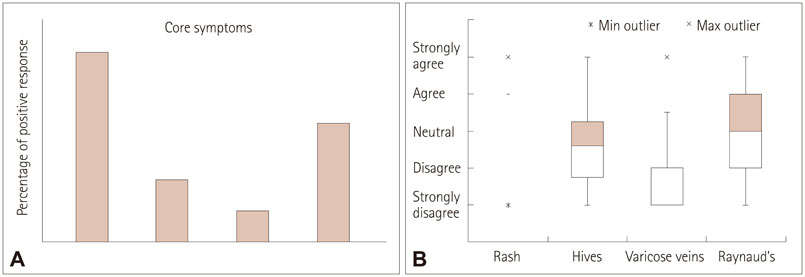
Fig. 1 Response rates for core dermatological symptoms. A: Bar graph displays the frequency of positive responses (i.e., "strongly agree" or "agree"). B: Box-and-whisker plots display the median and interquartile range for each symptom. Q1: first quartile, Q3: third quartile.
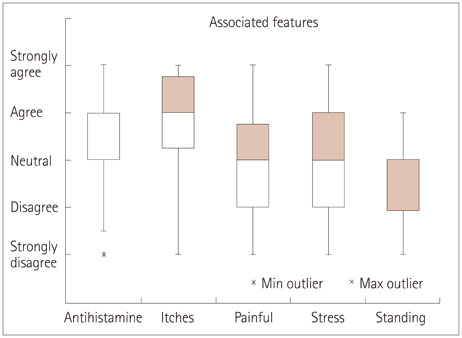
Fig. 2 Response rates for associated features of rash among subjects positive for "rash". Box-and-whisker plots display the median and interquartile range for each location. "Antihistamine"=no response to antihistamine medication.
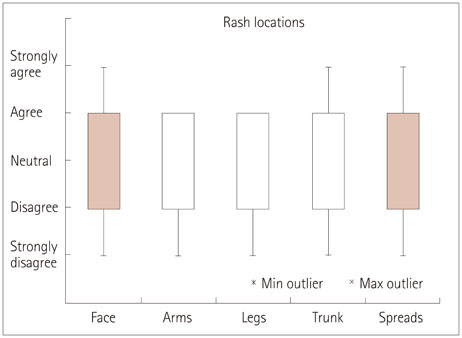
Fig. 3 Response rates for locations of rash among subjects positive for "rash". Box-and-whisker plots display the median and interquartile range for each location.
Reference
-
1. Stewart JM. Pooling in chronic orthostatic intolerance: arterial vasoconstrictive but not venous compliance defects. Circulation. 2002; 105:2274–2281.2. Schondorf R, Low PA. Idiopathic postural orthostatic tachycardia syndrome: an attenuated form of acute pandysautonomia? Neurology. 1993; 43:132–137.
Article3. Low PA, Opfer-Gehrking TL, Textor SC, Schondorf R, Suarez GA, Fealey RD, et al. Comparison of the postural tachycardia syndrome (POTS) with orthostatic hypotension due to autonomic failure. J Auton Nerv Syst. 1994; 50:181–188.
Article4. Benarroch EE. Postural tachycardia syndrome: a heterogeneous and multifactorial disorder. Mayo Clin Proc. 2012; 87:1214–1225.
Article5. Raj SR, Robertson D. Blood volume perturbations in the postural tachycardia syndrome. Am J Med Sci. 2007; 334:57–60.
Article6. Jordan J, Shannon JR, Diedrich A, Black BK, Robertson D. Increased sympathetic activation in idiopathic orthostatic intolerance: role of systemic adrenoreceptor sensitivity. Hypertension. 2002; 39:173–178.
Article7. Jacob G, Costa F, Shannon JR, Robertson RM, Wathen M, Stein M, et al. The neuropathic postural tachycardia syndrome. N Engl J Med. 2000; 343:1008–1014.
Article8. Joyner MJ, Masuki S. POTS versus deconditioning: the same or different? Clin Auton Res. 2008; 18:300–307.
Article9. Ojha A, Chelimsky TC, Chelimsky G. Comorbidities in pediatric patients with postural orthostatic tachycardia syndrome. J Pediatr. 2011; 158:20–23.
Article10. Landero J. Postural orthostatic tachycardia syndrome: a dermatologic perspective and successful treatment with losartan. J Clin Aesthet Dermatol. 2014; 7:41–47.11. Suter LG, Murabito JM, Felson DT, Fraenkel L. The incidence and natural history of Raynaud's phenomenon in the community. Arthritis Rheum. 2005; 52:1259–1263.
Article12. Maricq HR, Carpentier PH, Weinrich MC, Keil JE, Franco A, Drouet P, et al. Geographic variation in the prevalence of Raynaud's phenomenon: Charleston, SC, USA, vs Tarentaise, Savoie, France. J Rheumatol. 1993; 20:70–76.13. Stewart JM, Taneja I, Medow MS. Reduced body mass index is associated with increased angiotensin II in young women with postural tachycardia syndrome. Clin Sci (Lond). 2007; 113:449–457.
Article14. Stewart JM, Taneja I, Glover J, Medow MS. Angiotensin II type 1 receptor blockade corrects cutaneous nitric oxide deficit in postural tachycardia syndrome. Am J Physiol Heart Circ Physiol. 2008; 294:H466–H473.
Article15. Stewart JM, Ocon AJ, Clarke D, Taneja I, Medow MS. Defects in cutaneous angiotensin-converting enzyme 2 and angiotensin-(1-7) production in postural tachycardia syndrome. Hypertension. 2009; 53:767–774.
Article16. Greaves M. Chronic urticaria. J Allergy Clin Immunol. 2000; 105:664–672.
Article17. Shibao C, Arzubiaga C, Roberts LJ 2nd, Raj S, Black B, Harris P, et al. Hyperadrenergic postural tachycardia syndrome in mast cell activation disorders. Hypertension. 2005; 45:385–390.
Article18. Sharma M, Bennett C, Cohen SN, Carter B. H1-antihistamines for chronic spontaneous urticaria. Cochrane Database Syst Rev. 2014; 11:CD006137.
Article19. Shelley WB, Shelley ED. Adrenergic urticaria: a new form of stress-induced hives. Lancet. 1985; 2:1031–1033.
Article20. Haustein UF. Adrenergic urticaria and adrenergic pruritus. Acta Derm Venereol. 1990; 70:82–84.21. Chapman EM, Asmussen E. On the occurrence of dyspnea, dizziness and precordial distress ccasioned by the pooling of blood in varicose veins. J Clin Invest. 1942; 21:393–399.
Article22. National Clinical Guideline Centre (UK). Varicose Veins in the Legs: The Diagnosis and Management of Varicose Veins. London: National Institute for Health and Care Excellence (UK);2013.
