Video-Assisted Thoracoscopic Minimally Invasive Anterior Interbody Fusion of the T11-T12 Level Using Direct Lateral Interbody Fusion Devices: A Case Report
- Affiliations
-
- 1Department of Orthopaedic Surgery, Hanyang University College of Medicine, Seoul, Korea. cnkang65@hanyang.ac.kr
- 2Department of Orthopaedic Surgery, Sung-Ae Hospital, Seoul, Korea.
- KMID: 2353909
- DOI: http://doi.org/10.4184/jkss.2016.23.3.177
Abstract
- STUDY DESIGN: Case report
OBJECTIVES
To report a case of video-assisted thoracoscopic (VAT) minimally invasive anterior interbody fusion of the T11-T12 level using direct lateral interbody fusion (DLIF) devices. SUMMARY OF LITERATURE REVIEW: Interbody fusion of the thoracolumbar junction (especially T11-T12) is technically challenging from anterior, lateral, or posterior approaches. A VAT anterior interbody fusion approach using DLIF devices is a safe, minimally invasive alternative approach to the thoracolumbar spine.
MATERIALS AND METHODS
A 37-year-old male pedestrian was struck by a car sustaining fracture-dislocation at the T11-T12 level. The accident resulted in complete paraplegia of both lower extremities and multiple lower extremity fractures. A classical instrumented posterolateral fusion from T8 to L3 and staged VAT anterior interbody fusion at the T11-T12 level were performed.
RESULTS
At one year postoperatively, he was capable of independent ambulation using a wheelchair without back pain, and plain radiographs and CT scans showed a solid fusion at the T11-T12 level.
CONCLUSIONS
VAT anterior interbody fusion using DLIF devices provides excellent access to the anterior spinal column with the added benefits of an improved field of view and can be a safe and effective alternative to open thoracotomy in the management of various thoracolumbar junction problems.
Keyword
MeSH Terms
Figure
-
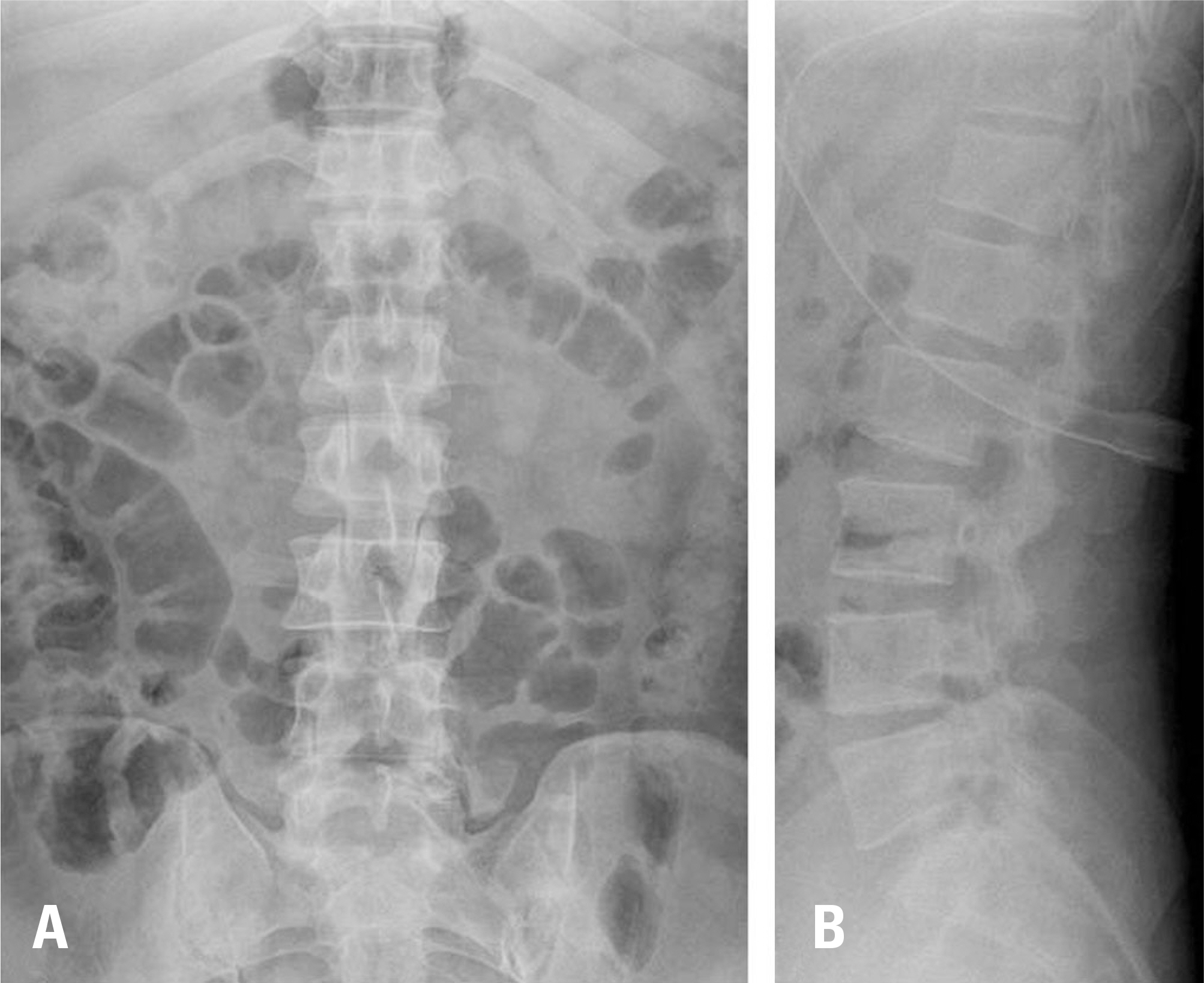
Fig. 1. The plain radiographs of 37-year-old male pedestrian, who was struck by a car, show fracture-dislocation injury at the T11-T12 level (A, B). The accident resulted in complete paraplegia of both lower extremities.

Fig. 2. Sagittal (A), coronal (B), and axial (C) computed tomography scans and magnetic resonance imaging (D) show fracture-dislocation injury at the T11-T12 level. A transection cord injury at the T11 body level, lateral displacement with intervertebral subluxation, and fracture at both superior articular processes of the T12 vertebra occurred.

Fig. 3. Lateral radiographs of the surgical site preoperatively (A) and after posterior operation (B) are shown. After the posterior operation, the T11-T12 interbody space was widened from 5 mm to 12 mm and facet joint subluxation still existed.
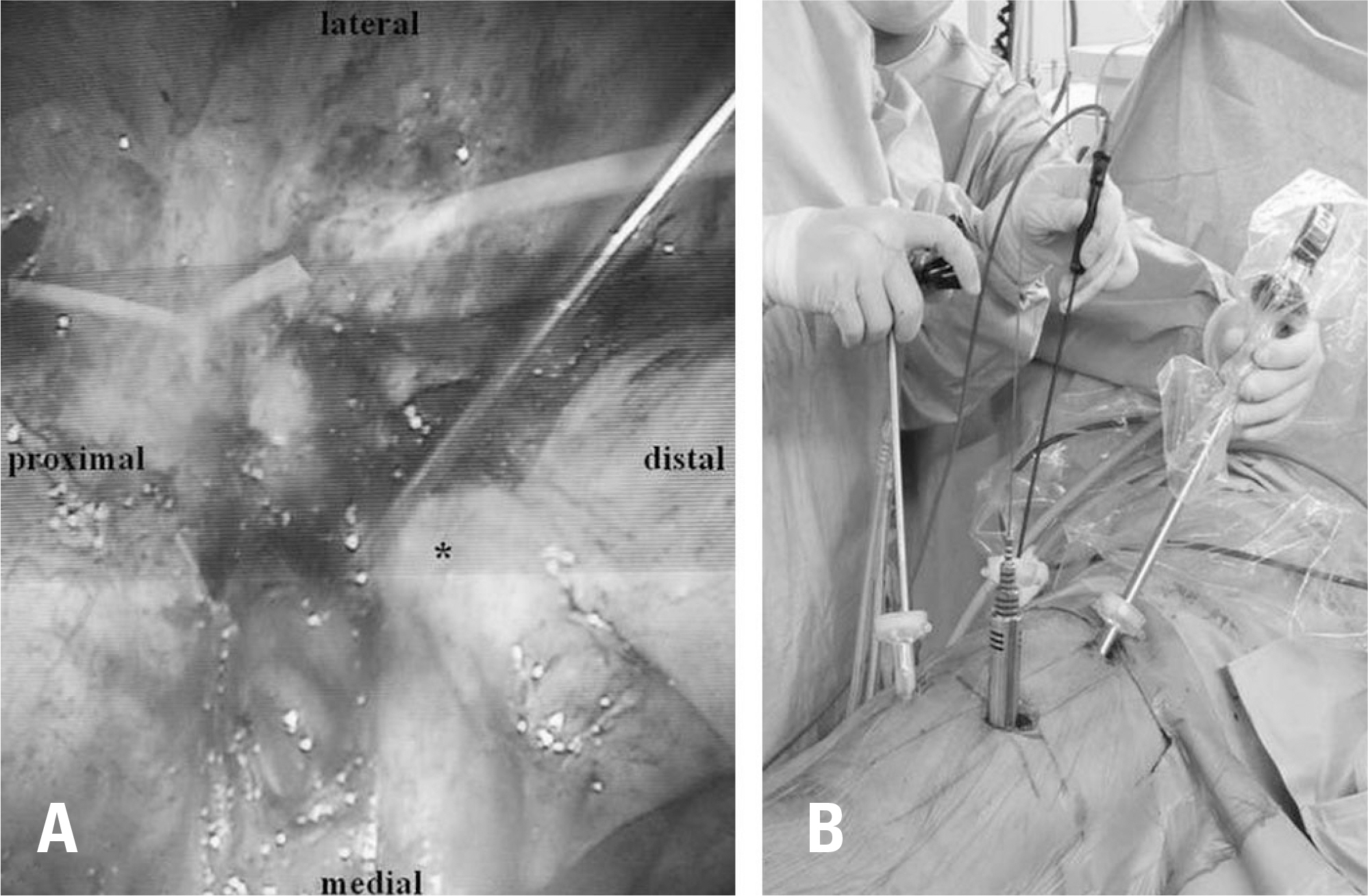
Fig. 4. A thoracoscopic image shows the T11-T12 level (A). The dia-phragm (asterisk) was detached from the chest wall to expose the T11-T12 interbody disc space. A guide pin was inserted at the T11-T12 interbody disc space. An intraoperative image is shown (B). Serial dila-tors were inserted directly lateral to the T11-T12 interbody disc space. A viewing camera and instruments for thoracoscopy were inserted via trocars.

Fig. 5. Postoperative anteroposterior (A) and lateral (B) plain radiographs show T8-L3 transpedicular fixation, T11-T12 interbody fusion, and posterolateral fusion. The postoperative 1 year coronal (C) and sagittal (D) CT scans show a solid bony union at the interbody space.
Reference
-
1. Lee CG, Choi JS, Kim YC, et al. Survival Analysis of Posterior Short Fusion in Thoracolumbar Fracture-Significance of Load-Sharing Score and Bone Mineral Density. J Korean Soc Spine Surg. 2001; 8:113–20.2. Wang X-B, Yang M, Li J, et al. Thoracolumbar fracture dislocations treated by posterior reduction, interbody fusion and segmental instrumentation. Indian J Orthop. 2014; 48:568–73.
Article3. Wood KB, Li W, Lebl DS, et al. Management of thoracolumbar spine fractures. Spine J. 2014; 14:145–64.
Article4. Xia Q, Xu Bs, Zhang Jd, et al. Simultaneous combined anterior and posterior surgery for severe thoracolumbar fracture dislocations. Orthop Surg. 2009; 1:28–33.
Article5. Machino M, Yukawa Y, Ito K, et al. Posterior/anterior combined surgery for thoracolumbar burst fractures— posterior instrumentation with pedicle screws and laminar hooks, anterior decompression and strut grafting. Spinal cord. 2011; 49:573–9.6. Yu S-W, Fang K-F, Tseng I-C, et al. Surgical Outcomes of Short-Segment Fixation for Thoracolumbar Fracture Dis-location. Chang Gung med J. 2002; 25:253–9.7. Rosenthal D. Endoscopic approaches to the thoracic spine. Eur Spine J. 2000; 9(Suppl):8–16.
Article8. Karikari IO, Nimjee SM, Hardin CA, et al. Extreme lateral interbody fusion approach for isolated thoracic and thoracolumbar spine diseases: initial clinical experience and early outcomes. J Spinal Disord Tech. 2011; 24:368–75.9. Meredith DS, Kepler CK, Huang RC, et al. Extreme lateral interbody fusion (XLIF) in the thoracic and thoracolumbar spine: technical report and early outcomes. HSS J. 2013; 9:25–31.
Article10. Levin R, Matusz D, Hasharoni A, et al. Mini-open tho-racoscopically assisted thoracotomy versus video-assisted thoracoscopic surgery for anterior release in thoracic scoliosis and kyphosis: a comparison of operative and radiographic results. Spine J. 2005; 5:632–8.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Minimally Invasive Lateral Lumbar Interbody Fusion: Indications, Outcomes and Complications
- Minimally Invasive Lateral Lumbar Interbody Fusion: Surgical Technique and Review
- Lateral Lumbar Interbody Fusion
- Contralateral Nerve Root Compression after Direct Lateral Lumbar Interbody Fusion
- A Prospective Comparison of Surgical Approach for Lateral Retroperitoneal L4-5 Fusion: Laparoscopic Versus Mini-ALIF
