Minimally Invasive Lateral Lumbar Interbody Fusion: Surgical Technique and Review
- Affiliations
-
- 1Department of Orthopedic Surgery, College of Medicine, Soonchunhyang University Cheonan Hospital, Korea.
- 2Department of Orthopedic Surgery, Spine Center, College of Medicine, Soonchunhyang University Hospital, Seoul, Korea. jlee@schmc.ac.kr
- KMID: 2365088
- DOI: http://doi.org/10.4184/jkss.2016.23.4.262
Abstract
- STUDY DESIGN: Review of the current surgical technique and literature.
OBJECTIVES
The aim of this study was to review the surgical technique and the current evidence on minimally invasive lateral lumbar interbody fusion (LLIF). SUMMARY OF LITERATURE REVIEW: Spinal fusion is a useful method in the treatment of various degenerative lumbar diseases. Recently, minimally invasive LLIF has been developed, enabling spine surgeons to perform anterior interbody fusion in a minimally invasive manner.
MATERIALS AND METHODS
Review of the surgical technique and the literature.
RESULTS
Minimally invasive LLIF may reduce the incidence of complications of anterior lumbar interbody fusion. LLIF may restore disc height more effectively than posterior lumbar interbody fusion and indirectly decompress the neural canal without nerve root or dural retraction or perineural scaring. The current indications for LLIF are almost equivalent to those of anterior and posterior lumbar interbody fusion. Recent studies have reported no differences in the fusion rate or clinical outcomes between LLIF and the conventional anterior or posterior interbody fusion techniques. However, LLIF has nonspecific complications, such as anterior thigh pain and hip flexor weakness.
CONCLUSIONS
Minimally invasive LLIF is a promising surgical alternative to the conventional anterior or posterior fusion techniques. LLIF has the advantages of less intraoperative bleeding and soft tissue injury, and a faster return to work. However, postoperative nonspecific complications are problems that need to be addressed.
MeSH Terms
Figure
-

Fig. 1. Preoperative lumbar bending radiographs show that the right-side approach to the L4-L5 disc space appears to be easier than the left-side approach (A) (see arrows). This evaluation is important, especially when the L4-L5 disc space is partially ob-structed by one of the iliac crests on lateral radiographs (B) (see arrows).

Fig. 2. A photograph shows the preoperative position of the patient. The posture of the patient is lateral on a bent operative table with hip and knee flexed.
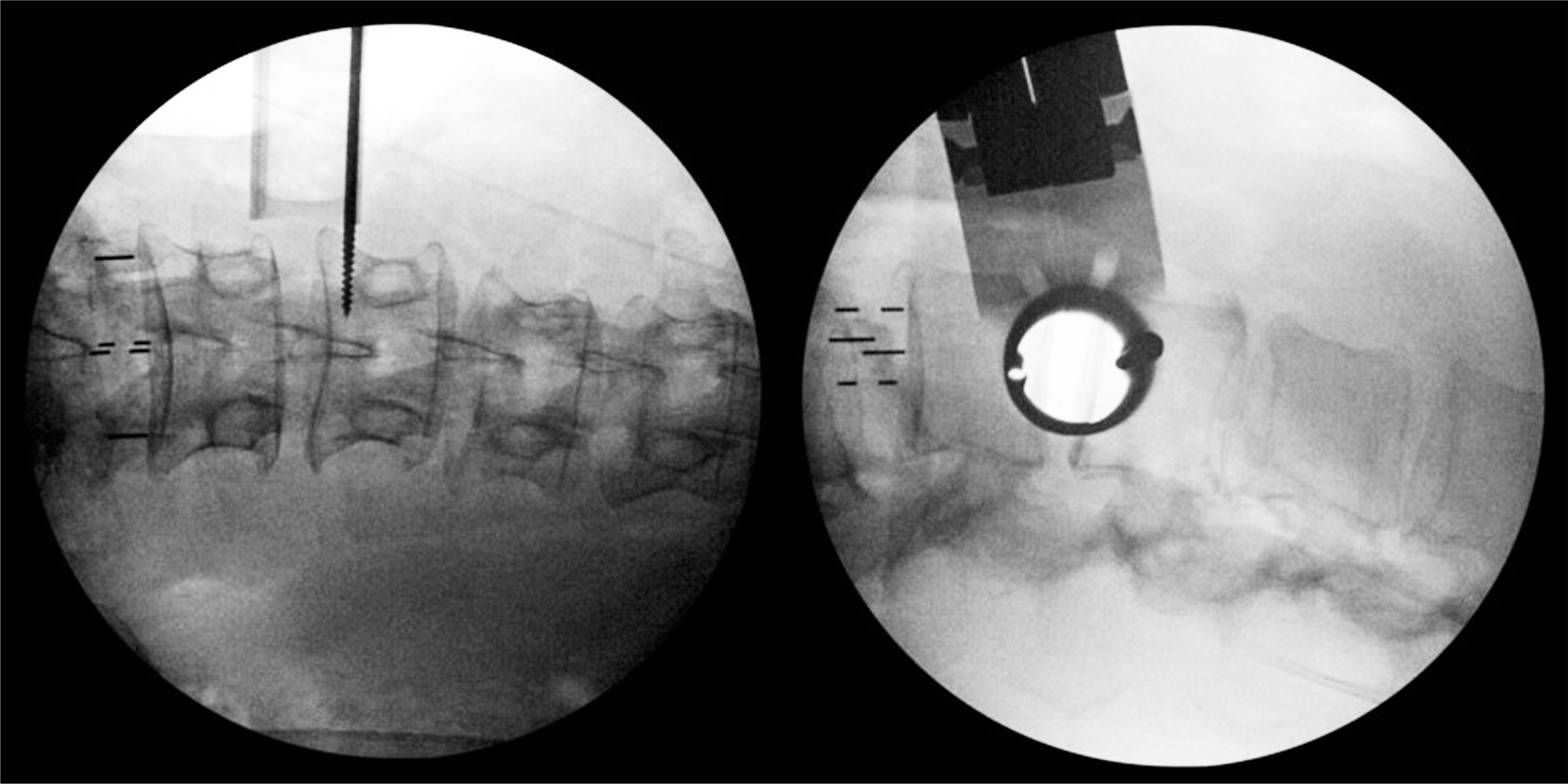
Fig. 3. Intraoperative fluoroscopic anteroposterior and lateral images show the optimal placement of the tubular retractor for the operation.
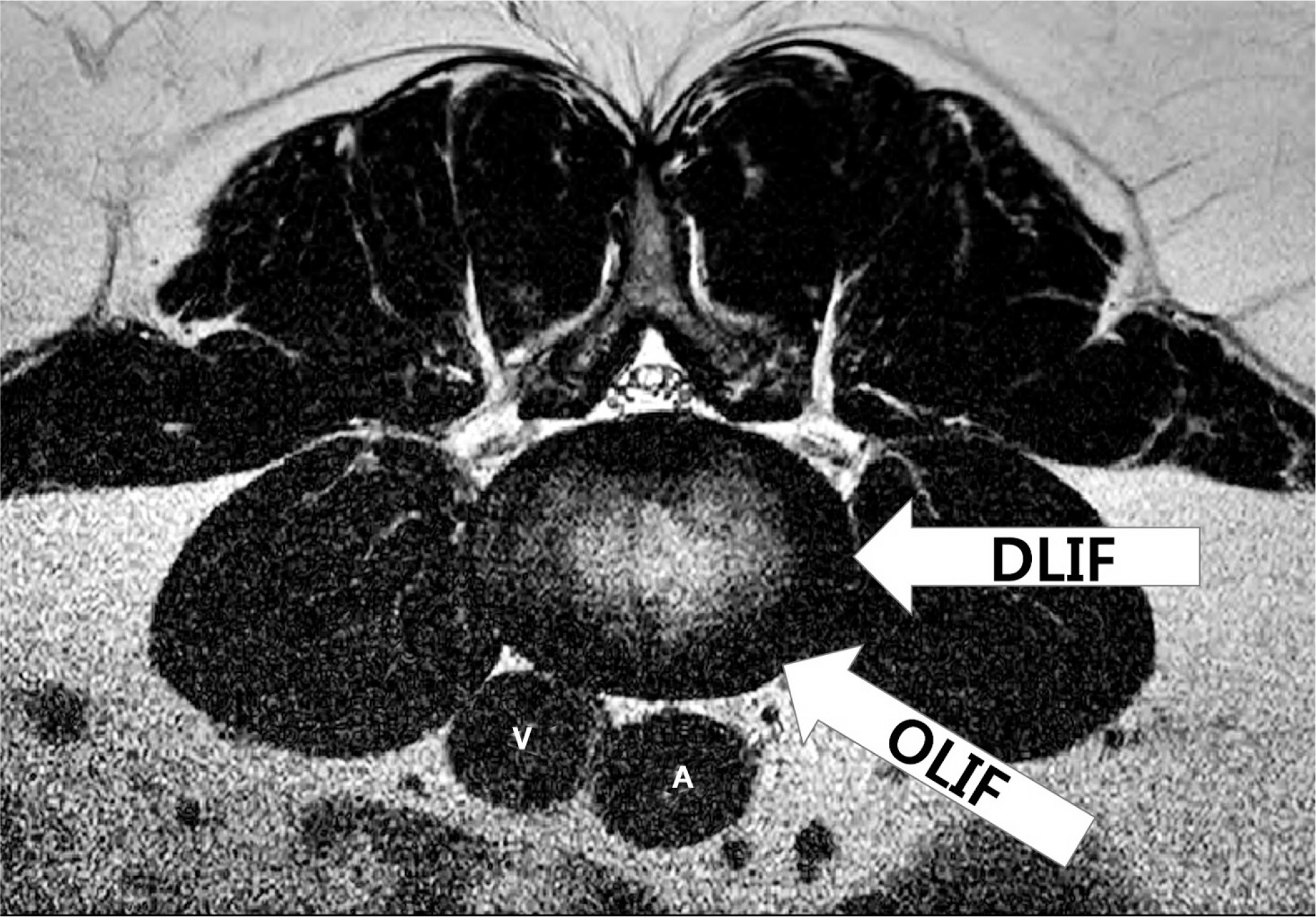
Fig. 4. A schematic figure shows the difference between the direct lateral interbody fusion and oblique lateral interbody fusion approaches for the lumbar spine (see arrows). A, abdominal aorta; V, vena cava.
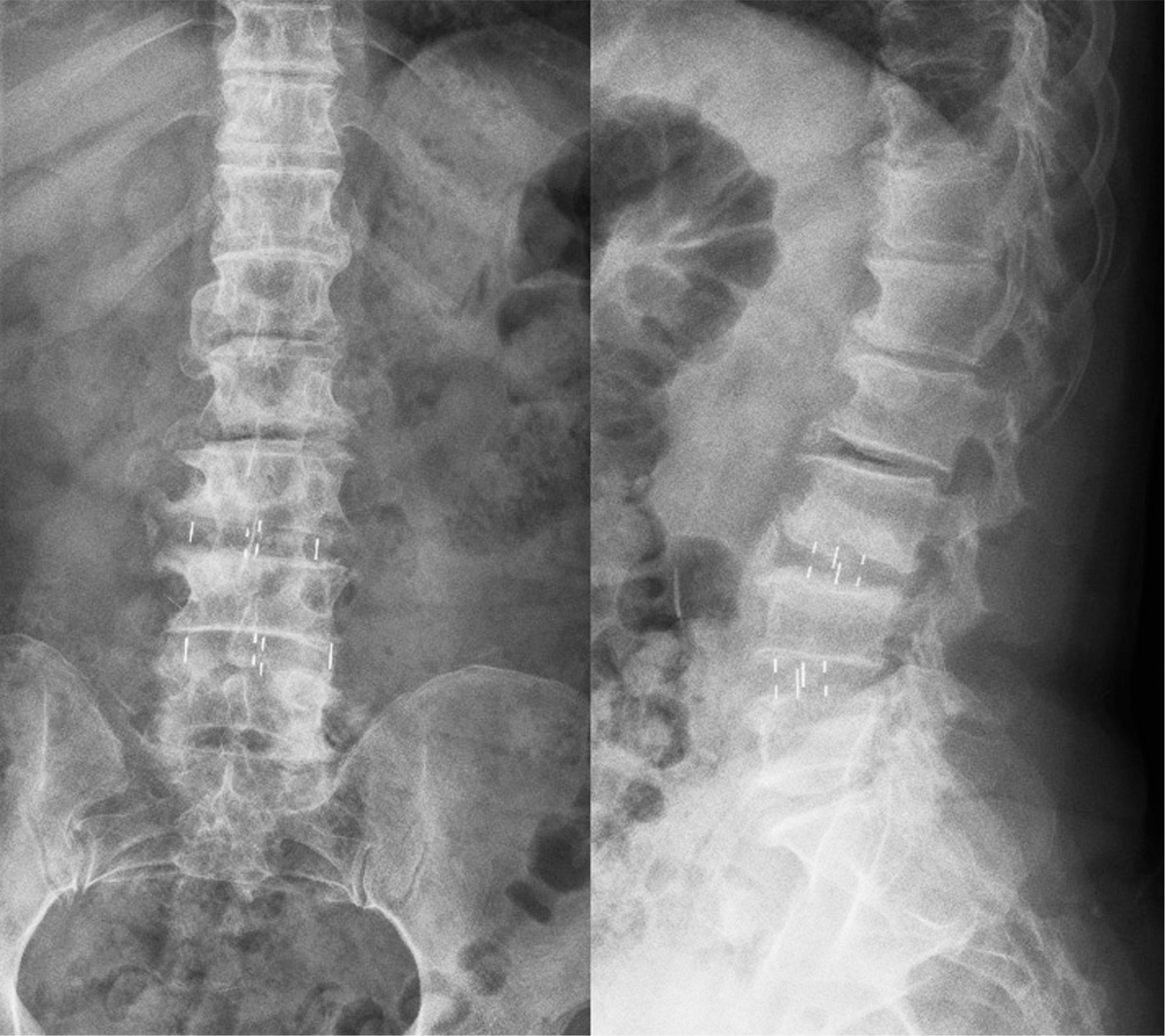
Fig. 5. Postoperative lumbar anteroposterior and lateral radiographs show the proper placement of cages.
Reference
-
1. Arnold PM, Anderson KK, McGuire RA Jr. The lateral transpsoas approach to the lumbar and thoracic spine: A review. Surg Neurol Int. 2012; 3(Suppl):198–215.
Article2. Ozgur BM, Aryan HE, Pimenta L, et al. Extreme lateral interbody fusion(XLIF): a novel surgical technique for anterior lumbar interbody fusion. Spine J. 2006; 6:435–43.3. Dakwar E, Cardona RF, Smith DA, et al. Early outcomes and safety of the minimally invasive, lateral retroperitoneal transpsoas approach for adult degenerative scoliosis. Neurosurg Focus. 2010; 28:E8.
Article4. Pawar A, Hughes A, Girardi F, et al. Lateral lumbar interbody fusion. Asian Spine J. 2015; 9:978–83.
Article5. Oliveira L, Marchi L, Coutinho E, et al. A radiographic assessment of the ability of the extreme lateral interbody fusion procedure to indirectly decompress the neural elements. Spine(Phila pa 1976). 2010; 35(Suppl):331–7.
Article6. Kim SJ, Lee YS, Kim YB, et al. Clinical and Radiological outcomes of New Cage for Direct Lateral Lumbar Inter-body Fusion. Korean J Spine. 2014; 11:145–51.7. Arnold PM, Anderson KK, McGuire RA Jr. The lateral transpsoas approach to the lumbar and thoracic spine: A review. Surg Neurol Int. 2012; 3(Suppl):198–215.
Article8. Mundis GM, Akbarnia BA, Phillips FM. Adult deformity correction through minimally invasive lateral approach techniques. Spine(Phila Pa 1976). 2010; 35(Suppl):312–21.
Article9. Acosta FL, Liu J, Slimack N, et al. Changes in coronal and sagittal plane alignment following minimally invasive direct lateral interbody fusion for the treatment of degenerative lumbar disease in adults: a radiographic study. J Neurosurg Spine. 2011; 15:92–6.
Article10. Phan K, Rao PJ, Scherman DB, et al. Lateral lumbar interbody fusion for sagittal balance correction and spinal deformity. J Clin Neurosci. 2015; 22:1714–21.
Article11. Benglis DM, Vanni S, Levi AD. An anatomical study of the lumbosacral plexus as related to the minimally invasive transpsoas approach to the lumbar spine. J Neurosurg Spine. 2009; 10:139–44.
Article12. Jahangiri FR, Sherman JH, Holmberg A, et al. Protecting the genitofemoral nerve during direct/extreme lateral interbody fusion (DLIF/XLIF) procedures. Am J Electroneuro-diagnostic Technol. 2010; 50:321–35.
Article13. Laws CJ, Coughlin DG, Lotz JC, et al. Direct lateral approach to lumbar fusion in a biomechanically equivalent alternative to the anterior approach: an in vitro study. Spine(Phila Pa 1976). 2012; 37:819–25.14. Frotzell P, Hagg O, Wessberg P, et al. Chronic low back pain and fusion: a comparison of three surgical techniques: a prospective multicenter randomized study from the Swedish lumbar spine study group. Spine(Phila Pa 1976). 2002; 27:1131–41.15. Christensen FB, Hansen ES, Ekskjaer SP, et al. Circum-ferential lumbar spinal fusion with Brantigan cage versus posterolateral fusion with titanium Cotrel-Dubousset instrumentation: a prospective, randomized clinical study of 146 patients. Spine(Phila Pa 1976). 2002; 27:2674–83.16. Hackenberg L, Halm H, Bullmann V, et al. Transforaminal lumbar interbody fusion: a safe technique with satisfactory three to five year results. Eur Spine J. 2005; 14:551–8.
Article17. Bono CM, Lee CK. Critical analysis of trends in fusion for degenerative disc disease over the past 20 years: influence of technique on fusion rate and clinical outcome. Spine(Phila Pa 1976). 2004; 29:455–63.18. Watkins R 4th, Watkins R 3rd, Hanna R. Non-union rate with standalone lateral lumbar interbody fusion. Medicine(Baltimore). 2014; 93:E275.
Article19. Berjano P, Langella F, Damilano M, et al. Fusion rate following extreme lateral lumbar interbody fusion. Eur Spine J. 2015; 24(Suppl):369–71.
Article20. Marchi L, Abdala N, Oliveira L, et al. Radiographic and clinical evaluation of cage subsidence after standalone lateral interbody fusion. J Neurosurg Spine. 2013; 19:110–8.
Article21. Kretzer RM, Molina C, Hu N, et al. A comparative biomechanical analysis of stand alone versus facet screw and pedicle screw augmented lateral interbody arthrodesis: An in vitro human cadaveric model. Clin Spine Surg. 2016; 29:E336–43.22. Cappuccino A, Cornwall GB, Turner AW, et al. Biomechanical analysis and review of lateral lumbar fusion con-structs. Spine(Phila Pa 1976). 2010; 35(Suppl):361–7.
Article23. Guerin P, Obeid I, Bourghli A, et al. The lumbosacral plexus: anatomic considerations for minimally invasive retroperitoneal transpsoas approach. Surg Radiol Anat. 2012; 34:151–7.
Article24. Kepler CK, Bogner EA, Herzog RJ, et al. Anatomy of the psoas muscle and lumbar plexus with respect to the surgical approach for lateral transpsoas interbody fusion. Eur Spine J. 2011; 20:550–6.
Article25. Sharma AK, Kepler CK, Girardi FP, et al. Lateral lumbar interbody fusion: clinical and radiographic outcomes at 1 year: a preliminary report. J Spinal Disord Tech. 2011; 24:242–50.26. Pumberger M, Hughes AP, Huang RR, et al. Neurologic deficit following lateral lumbar interbody fusion. Eur Spine J. 2012; 21:1192–9.
Article27. Dakwar E, Le TV, Baaj AA, et al. Abdominal wall paresis as a complication of minimal invasive lateral transpsoas interbody fusion. Neurosurg Focus. 2011; 31:E18.28. Karikari IO, Grossi PM, Nimjee SM, et al. Minimally inva-sive lumbar interbody fusion in patients older than 70 years of age: analysis of peri- and postoperative complications. Neurosurgery. 2011; 68:897–902.
Article29. Brier-Jones JE, Palmer DK, Inceoglu S, et al. Vertebral body fractures after transpsoas interbody fusion procedures. Spine J. 2011; 11:1068–72.
Article30. Beckman JM, Vincent B, Park MS, et al. Contralateral psoas hematoma after minimally invasive, lateral retroperitoneal transpsoas lumbar interbody fusion: a multicenter review of 3950 lumbar levels. J Neurosurg Spine. 2016; 5:1–5.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Minimally Invasive Lateral Lumbar Interbody Fusion: Indications, Outcomes and Complications
- Biportal Endoscopic Transforaminal Interbody Fusion for Lumbar Adjacent Segment Disease: An Illustrative Case and Literature Review
- Pearls and Pitfalls of Oblique Lateral Interbody Fusion: A Comprehensive Narrative Review
- Minimally Invasive Strategy for Uniportal Full-Endoscopic Transforaminal Lumbar Interbody Fusion Using a Large Cage Utilized in Oblique Lumbar Interbody Fusion
- Lateral Lumbar Interbody Fusion
