Pediatr Infect Vaccine.
2016 Aug;23(2):109-116. 10.14776/piv.2016.23.2.109.
Vitamin D and Risk of Respiratory Tract Infections in Children: A Systematic Review and Meta-analysis of Randomized Controlled Trials
- Affiliations
-
- 1Department of Pediatrics, Ewha Medical Research Institute, Ewha Womans University School of Medicine, Seoul, Korea. kaykim@ewha.ac.kr
- 2Center for Vaccine Evaluation and Study, Ewha Medical Research Institute, Ewha Womans University School of Medicine, Seoul, Korea.
- KMID: 2353391
- DOI: http://doi.org/10.14776/piv.2016.23.2.109
Abstract
- PURPOSE
Recent observational studies have found that vitamin D deficiency is associated with respiratory tract infections. However, randomized controlled trials (RCTs) regarding the efficacy of vitamin D in childhood respiratory tract infection (RTI) have yield inconsistent results. We performed a systematic review and meta-analysis to evaluate the association between vitamin D supplementation and the risk of RTI.
METHODS
A comprehensive search was conducted using MEDLINE, EMBASE, and the Cochrane Central Register of Controlled Trial. Randomized controlled trials of vitamin D supplementation for prevention of RTI in children were included for the analysis. Cochrane Collaboration's tool for assessing the risk of bias was used to assess the quality of the studies. Pooled risk ratios with 95% confidence intervals (CIs) were meta-analyzed using Review Manager 5.3.
RESULTS
A total of seven RCTs were included in the meta-analysis. According to a random-effects model, the risk ratio for vitamin D supplementation was 0.82 (95% CI: 0.69-0.98) and I2=62% for heterogeneity. On subgroup analysis, heterogeneity decreased in the subgroup with follow-up less than 1 year, participants ≥5 years of age, patients subgroup, and subgroup with dosing daily. Funnel plot showed that there might be publication bias in the field.
CONCLUSIONS
The present meta-analysis supports a beneficial effect of vitamin D supplementation for the prevention of RTI in children. However, the result should be interpreted with caution due to limitations including a small number of available RCTs, heterogeneity among the studies, and potential publication bias.
MeSH Terms
Figure
-
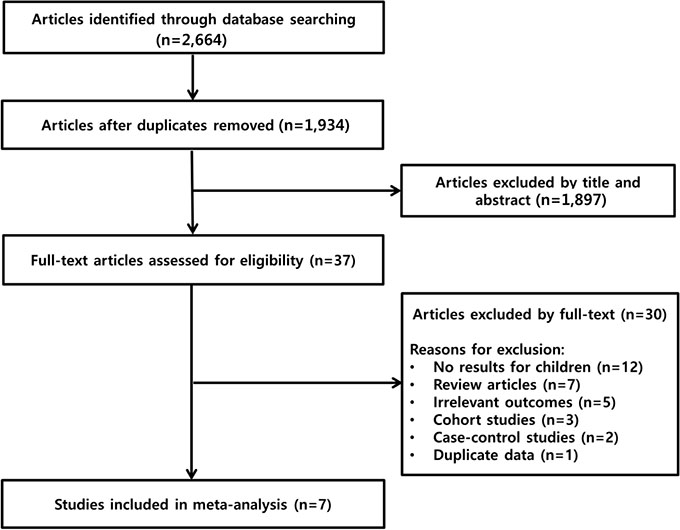
Fig. 1 Flow chart for selection of eligible studies.

Fig. 2 Forest plot of vitamin D supplementation effects for prevention of respiratory tract infections.
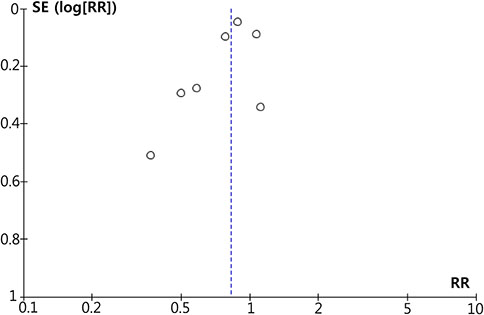
Fig. 3 Funnel plot of included studies. SE, standard error, RR, risk ratio.
Reference
-
1. Wang TT, Nestel FP, Bourdeau V, Nagai Y, Wang Q, Liao J, et al. Cutting edge: 1,25-dihydroxyvitamin D3 is a direct inducer of antimicrobial peptide gene expression. J Immunol. 2004; 173:2909–2912.
Article2. Bikle D. Nonclassic actions of vitamin D. J Clin Endocrinol Metab. 2009; 94:26–34.
Article3. Liu PT, Stenger S, Li H, Wenzel L, Tan BH, Krutzik SR, et al. Toll-like receptor triggering of a vitamin D-mediated human antimicrobial response. Science. 2006; 311:1770–1773.
Article4. Liu PT, Stenger S, Tang DH, Modlin RL. Cutting edge: vitamin D-mediated human antimicrobial activity against Mycobacterium tuberculosis is dependent on the induction of cathelicidin. J Immunol. 2007; 179:2060–2063.
Article5. Nimmerjahn F, Dudziak D, Dirmeier U, Hobom G, Riedel A, Schlee M, et al. Active NF-kappaB signalling is a prerequisite for influenza virus infection. J Gen Virol. 2004; 85:2347–2356.6. Hansdottir S, Monick MM, Lovan N, Powers L, Gerke A, Hunninghake GW. Vitamin D decreases respiratory syncytial virus induction of NF-kappaB-linked chemokines and cytokines in airway epithelium while maintaining the antiviral state. J Immunol. 2010; 184:965–974.
Article7. Mahon BD, Wittke A, Weaver V, Cantorna MT. The targets of vitamin D depend on the differentiation and activation status of CD4 positive T cells. J Cell Biochem. 2003; 89:922–932.
Article8. Nashold FE, Hoag KA, Goverman J, Hayes CE. Rag-1-dependent cells are necessary for 1,25-dihydroxyvitamin D(3) prevention of experimental autoimmune encephalomyelitis. J Neuroimmunol. 2001; 119:16–29.
Article9. Jolliffe DA, Griffiths CJ, Martineau AR. Vitamin D in the prevention of acute respiratory infection: systematic review of clinical studies. J Steroid Biochem Mol Biol. 2013; 136:321–329.
Article10. Wayse V, Yousafzai A, Mogale K, Filteau S. Association of subclinical vitamin D deficiency with severe acute lower respiratory infection in Indian children under 5 y. Eur J Clin Nutr. 2004; 58:563–567.
Article11. Karatekin G, Kaya A, Salihoglu O, Balci H, Nuhoglu A. Association of subclinical vitamin D deficiency in newborns with acute lower respiratory infection and their mothers. Eur J Clin Nutr. 2009; 63:473–477.
Article12. Roth DE, Shah R, Black RE, Baqui AH. Vitamin D status and acute lower respiratory infection in early childhood in Sylhet, Bangladesh. Acta Paediatr. 2010; 99:389–393.
Article13. Camargo CA Jr, Ingham T, Wickens K, Thadhani R, Silvers KM, Epton MJ, et al. Cord-blood 25-hydroxyvitamin D levels and risk of respiratory infection, wheezing, and asthma. Pediatrics. 2011; 127:e180–e187.
Article14. Mohamed WA, Al-Shehri MA. Cord blood 25-hydroxyvitamin D levels and the risk of acute lower respiratory tract infection in early childhood. J Trop Pediatr. 2013; 59:29–35.
Article15. Belderbos ME, Houben ML, Wilbrink B, Lentjes E, Bloemen EM, Kimpen JL, et al. Cord blood vitamin D deficiency is associated with respiratory syncytial virus bronchiolitis. Pediatrics. 2011; 127:e1513–e1520.
Article16. Luczynska A, Logan C, Nieters A, Elgizouli M, Schottker B, Brenner H, et al. Cord blood 25(OH)D levels and the subsequent risk of lower respiratory tract infections in early childhood: the Ulm birth cohort. Eur J Epidemiol. 2014; 29:585–594.
Article17. Shin YH, Yu J, Kim KW, Ahn K, Hong SA, Lee E, et al. Association between cord blood 25-hydroxyvitamin D concentrations and respiratory tract infections in the first 6 months of age in a Korean population: a birth cohort study (COCOA). Korean J Pediatr. 2013; 56:439–445.
Article18. Bergman P, Lindh AU, Björkhem-Bergman L, Lindh JD. Vitamin D and respiratory tract infections: a systematic review and meta-analysis of randomized controlled trials. PloS one. 2013; 8:e65835.
Article19. Charan J, Goyal JP, Saxena D, Yadav P. Vitamin D for prevention of respiratory tract infections: a systematic review and meta-analysis. J Pharmacol Pharmacother. 2012; 3:300–303.
Article20. Xiao L, Xing C, Yang Z, Xu S, Wang M, Du H, et al. Vitamin D supplementation for the prevention of childhood acute respiratory infections: a systematic review of randomised controlled trials. Br J Nutr. 2015; 114:1026–1034.
Article21. Higgins JP, Altman DG, Gotzsche PC, Juni P, Moher D, Oxman AD, et al. The cochrane collaboration's tool for assessing risk of bias in randomised trials. BMJ. 2011; 343:d5928.
Article22. Borenstein M, Hedges LV, Higgins JP, Rothstein HR. A basic introduction to fixed-effect and random-effects models for meta-analysis. Res Synth Methods. 2010; 1:97–111.
Article23. Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002; 21:1539–1558.
Article24. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003; 327:557–560.
Article25. Oxman AD, Guyatt GH. A consumer's guide to subgroup analyses. Ann Intern Med. 1992; 116:78–84.
Article26. Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997; 315:629–634.
Article27. Kimball S, Vieth R, Dosch HM, Bar-Or A, Cheung R, Gagne D, et al. Cholecalciferol plus calcium suppresses abnormal PBMC reactivity in patients with multiple sclerosis. J Clin Endocrinol Metab. 2011; 96:2826–2834.
Article28. Camargo CA Jr, Ganmaa D, Frazier AL, Kirchberg FF, Stuart JJ, Kleinman K, et al. Randomized trial of vitamin D supplementation and risk of acute respiratory infection in Mongolia. Pediatrics. 2012; 130:e561–e567.
Article29. Grant CC, Kaur S, Waymouth E, Mitchell EA, Scragg R, Ekeroma A, et al. Reduced primary care respiratory infection visits following pregnancy and infancy vitamin D supplementation: a randomised controlled trial. Acta Paediatr. 2015; 104:396–404.
Article30. Majak P, Olszowiec-Chlebna M, Smejda K, Stelmach I. Vitamin D supplementation in children may prevent asthma exacerbation triggered by acute respiratory infection. J Allergy Clin Immunol. 2011; 127:1294–1296.
Article31. Manaseki-Holland S, Qader G, Isaq Masher M, Bruce J, Zulf Mughal M, Chandramohan D, et al. Effects of vitamin D supplementation to children diagnosed with pneumonia in Kabul: a randomised controlled trial. Trop Med Int Health. 2010; 15:1148–1155.
Article32. Manaseki-Holland S, Maroof Z, Bruce J, Mughal MZ, Masher MI, Bhutta ZA, et al. Effect on the incidence of pneumonia of vitamin D supplementation by quarterly bolus dose to infants in Kabul: a randomised controlled superiority trial. Lancet. 2012; 379:1419–1427.
Article33. Urashima M, Segawa T, Okazaki M, Kurihara M, Wada Y, Ida H. Randomized trial of vitamin D supplementation to prevent seasonal influenza A in schoolchildren. Am J Clin Nutr. 2010; 91:1255–1260.
Article34. Urashima M, Mezawa H, Noya M, Camargo CA Jr. Effects of vitamin D supplements on influenza A illness during the 2009 H1N1 pandemic: a randomized controlled trial. Food Funct. 2014; 5:2365–2370.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Maternal Vitamin D Supplementation for the Prevention of Respiratory Tract Infections in Offspring: A Meta-Analysis
- Introduction to systematic review and meta-analysis
- Effects of Vitamin D Supplementation on Children with Autism Spectrum Disorder: A Systematic Review and Meta-analysis
- Efficacy of Vitamin C Supplements in Prevention of Cancer: A Meta-Analysis of Randomized Controlled Trials
- Could Vitamin E Prevent Contrast-Induced Acute Kidney Injury? A Systematic Review and Meta-Analysis
