Evaluation of stability after pre-orthodontic orthognathic surgery using cone-beam computed tomography: A comparison with conventional treatment
- Affiliations
-
- 1Department of Orthodontics, College of Dentistry, Yonsei University, Seoul, Korea. BAIK@yuhs.ac
- 2Department of Oral and Maxillofacial Surgery, Oral Science Research center, College of Dentistry, Yonsei University, Seoul, Korea.
- 3The Institute of Craniofacial Deformity, College of Dentistry, Yonsei University, Seoul, Korea.
- KMID: 2352292
- DOI: http://doi.org/10.4041/kjod.2016.46.5.301
Abstract
OBJECTIVE
The aim of this study was to evaluate the skeletal and dental changes after intraoral vertical ramus osteotomy (IVRO) with and without presurgical orthodontics by using cone-beam computed tomography (CBCT).
METHODS
This retrospective cohort study included 24 patients (mean age, 22.1 years) with skeletal Class III malocclusion who underwent bimaxillary surgery with IVRO. The patients were divided into the preorthodontic orthognathic surgery (POGS) group (n = 12) and conventional surgery (CS) group (n = 12). CBCT images acquired preoperatively, 1 month after surgery, and 1 year after surgery were analyzed to compare the intergroup differences in postoperative three-dimensional movements of the maxillary and mandibular landmarks and the changes in lateral cephalometric variables.
RESULTS
Baseline demographics (sex and age) were similar between the two groups (6 men and 6 women in each group). During the postsurgical period, the POGS group showed more significant upward movement of the mandible (p < 0.05) than did the CS group. Neither group showed significant transverse movement of any of the skeletal landmarks. Moreover, none of the dental and skeletal variables showed significant intergroup differences 1 year after surgery.
CONCLUSIONS
Compared with CS, POGS with IVRO resulted in significantly different postsurgical skeletal movement in the mandible. Although both groups showed similar skeletal and dental outcomes at 1 year after surgery, upward movement of the mandible during the postsurgical period should be considered to ensure a more reliable outcome after POGS.
Keyword
MeSH Terms
Figure
-
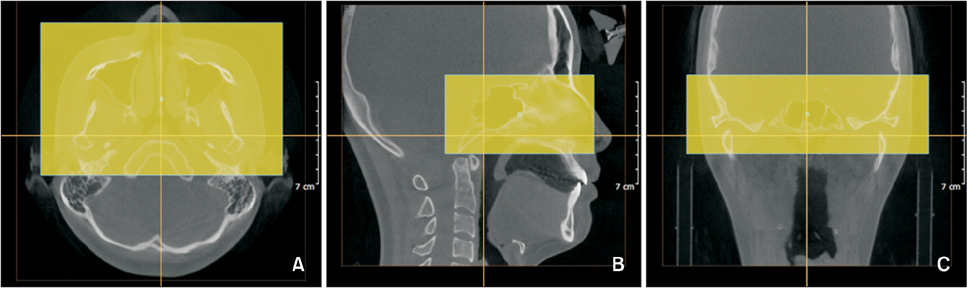
Figure 1 Superimposition of three-dimensional cone-beam computed tomography images with the cranial base structures by using the OnDemand3D software (CyberMed Inc., Seoul, Korea). The boxes indicate the areas of superimposition. A, Axial view; B, sagittal view; C, coronal view.
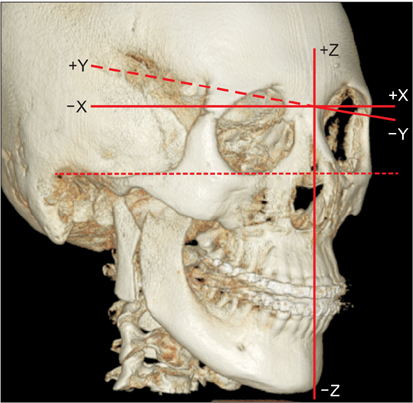
Figure 2 Coordinate system and zero point (Nasion). X-axis: (+) left, (−) right; Y-axis: (+) posterior, (−) anterior; Z-axis: (+) superior, (−) inferior.

Figure 3 Hard-tissue landmarks. The description of the landmarks is shown in Table 2.
Cited by 2 articles
-
Comparison of changes in the transverse dental axis between patients with skeletal Class III malocclusion and facial asymmetry treated by orthognathic surgery with and without presurgical orthodontic treatment
Han-Sol Song, Sung-Hwan Choi, Jung-Yul Cha, Kee-Joon Lee, Hyung-Seog Yu
Korean J Orthod. 2017;47(4):256-267. doi: 10.4041/kjod.2017.47.4.256.Three-dimensional structural analysis of the morphological condition of the alveolar bone before and after orthodontic treatment
Yasuhiro Shimizu, Takashi Ono
Korean J Orthod. 2017;47(6):394-400. doi: 10.4041/kjod.2017.47.6.394.
Reference
-
1. Nagasaka H, Sugawara J, Kawamura H, Nanda R. "Surgery first" skeletal Class III correction using the Skeletal Anchorage System. J Clin Orthod. 2009; 43:97–105.2. Villegas C, Uribe F, Sugawara J, Nanda R. Expedited correction of significant dentofacial asymmetry using a "surgery first" approach. J Clin Orthod. 2010; 44:97–103. quiz 105.3. Liou EJ, Chen PH, Wang YC, Yu CC, Huang CS, Chen YR. Surgery-first accelerated orthognathic surgery: postoperative rapid orthodontic tooth movement. J Oral Maxillofac Surg. 2011; 69:781–785.
Article4. Hernández-Alfaro F, Guijarro-Martínez R, Peiró-Guijarro MA. Surgery first in orthognathic surgery: what have we learned? A comprehensive workflow based on 45 consecutive cases. J Oral Maxillofac Surg. 2014; 72:376–390.
Article5. Min BK, Choi JY, Baek SH. Comparison of treatment duration between conventional three-stage method and surgery-first approach in patients with skeletal Class III malocclusion. J Craniofac Surg. 2014; 25:1752–1756.
Article6. Lee NK, Kim YK, Yun PY, Kim JW. Evaluation of post-surgical relapse after mandibular setback surgery with minimal orthodontic preparation. J Craniomaxillofac Surg. 2013; 41:47–51.
Article7. Kim JW, Lee NK, Yun PY, Moon SW, Kim YK. Postsurgical stability after mandibular setback surgery with minimal orthodontic preparation following upper premolar extraction. J Oral Maxillofac Surg. 2013; 71:1968.e1–1968.e11.
Article8. Kim CS, Lee SC, Kyung HM, Park HS, Kwon TG. Stability of mandibular setback surgery with and without presurgical orthodontics. J Oral Maxillofac Surg. 2014; 72:779–787.
Article9. Ko EW, Lin SC, Chen YR, Huang CS. Skeletal and dental variables related to the stability of orthognathic surgery in skeletal Class III malocclusion with a surgery-first approach. J Oral Maxillofac Surg. 2013; 71:e215–e223.
Article10. Joh B, Bayome M, Park JH, Park JU, Kim Y, Kook YA. Evaluation of minimal versus conventional presurgical orthodontics in skeletal class III patients treated with two-jaw surgery. J Oral Maxillofac Surg. 2013; 71:1733–1741.
Article11. Ko EW, Hsu SS, Hsieh HY, Wang YC, Huang CS, Chen YR. Comparison of progressive cephalometric changes and postsurgical stability of skeletal Class III correction with and without presurgical orthodontic treatment. J Oral Maxillofac Surg. 2011; 69:1469–1477.
Article12. Liao YF, Chiu YT, Huang CS, Ko EW, Chen YR. Presurgical orthodontics versus no presurgical orthodontics: treatment outcome of surgical-orthodontic correction for skeletal class III open bite. Plast Reconstr Surg. 2010; 126:2074–2083.
Article13. Choi JW, Lee JY, Yang SJ, Koh KS. The reliability of a surgery-first orthognathic approach without presurgical orthodontic treatment for skeletal class III dentofacial deformity. Ann Plast Surg. 2015; 74:333–341.
Article14. Choi SH, Hwang CJ, Baik HS, Jung YS, Lee KJ. Stability of pre-orthodontic orthognathic surgery using intraoral vertical ramus osteotomy versus conventional treatment. J Oral Maxillofac Surg. 2016; 74:610–619.
Article15. Gribel BF, Gribel MN, Frazäo DC, McNamara JA Jr, Manzi FR. Accuracy and reliability of craniometric measurements on lateral cephalometry and 3D measurements on CBCT scans. Angle Orthod. 2011; 81:26–35.
Article16. Chang ZC, Hu FC, Lai E, Yao CC, Chen MH, Chen YJ. Landmark identification errors on cone-beam computed tomography-derived cephalograms and conventional digital cephalograms. Am J Orthod Dentofacial Orthop. 2011; 140:e289–e297.
Article17. Cevidanes LH, Bailey LJ, Tucker SF, Styner MA, Mol A, Phillips CL, et al. Three-dimensional cone-beam computed tomography for assessment of mandibular changes after orthognathic surgery. Am J Orthod Dentofacial Orthop. 2007; 131:44–50.
Article18. Cevidanes LH, Motta A, Proffit WR, Ackerman JL, Styner M. Cranial base superimposition for 3-dimensional evaluation of soft-tissue changes. Am J Orthod Dentofacial Orthop. 2010; 137:4 Suppl. S120–S129.
Article19. Rhee CH, Choi YK, Kim YI, Kim SS, Park SB, Son WS. Correlation between skeletal and dental changes after mandibular setback surgery-first orthodontic treatment: Cone-beam computed tomography-generated half-cephalograms. Korean J Orthod. 2015; 45:59–65.
Article20. Chen CM, Lai SS, Wang CH, Wu JH, Lee KT, Lee HE. The stability of intraoral vertical ramus osteotomy and factors related to skeletal relapse. Aesthetic Plast Surg. 2011; 35:192–197.
Article21. Abeltins A, Jakobsone G, Urtane I, Bigestans A. The stability of bilateral sagittal ramus osteotomy and vertical ramus osteotomy after bimaxillary correction of class III malocclusion. J Craniomaxillofac Surg. 2011; 39:583–587.
Article22. Greebe RB, Tuinzing DB. Overcorrection and relapse after the intraoral vertical ramus osteotomy. A one-year postoperative review of thirty-five patients. Oral Surg Oral Med Oral Pathol. 1982; 54:382–384.
Article23. Jung HD, Jung YS, Kim SY, Kim DW, Park HS. Postoperative stability following bilateral intraoral vertical ramus osteotomy based on amount of setback. Br J Oral Maxillofac Surg. 2013; 51:822–826.
Article24. Choi SH, Kang DY, Cha JY, Jung YS, Yu HS, Park HS, et al. Major factors contributing to anterior and posterior relapse after intraoral vertical ramus osteotomy. J Craniomaxillofac Surg. 2016; 44:413–420.
Article25. Im J, Kang SH, Lee JY, Kim MK, Kim JH. Surgery-first approach using a three-dimensional virtual setup and surgical simulation for skeletal Class III correction. Korean J Orthod. 2014; 44:330–341.
Article26. Kim JY, Jung HD, Kim SY, Park HS, Jung YS. Postoperative stability for surgery-first approach using intraoral vertical ramus osteotomy: 12 month follow-up. Br J Oral Maxillofac Surg. 2014; 52:539–544.
Article27. Nihara J, Takeyama M, Takayama Y, Mutoh Y, Saito I. Postoperative changes in mandibular prognathism surgically treated by intraoral vertical ramus osteotomy. Int J Oral Maxillofac Surg. 2013; 42:62–70.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Surgical Stent Fabrication and Clinical Application for Orthognathic Surgery Using Cone-Beam CT
- Three-dimensional imaging modalities in endodontics
- Three-dimensional structural analysis of the morphological condition of the alveolar bone before and after orthodontic treatment
- Management of root canal perforation by using cone-beam computed tomography
- Clinical changes of TMD and condyle stability after two jaw surgery with and without preceding TMD treatments in class III patients
