Massive Calcified Cerebellar Pilocytic Astrocytoma with Rapid Recurrence : A Rare Case
- Affiliations
-
- 1Department of Neurosurgery, Baskent University Training and Research Hospital, Adana, Turkey. md.fatihaydemir@gmail.com
- 2Department of Pathology, Baskent University Training and Research Hospital, Adana, Turkey.
- KMID: 2351726
- DOI: http://doi.org/10.3340/jkns.2016.59.5.533
Abstract
- Pilocytic astrocytomas (PAs) are World Heath Organization Grade I tumors and are most common in children. PA calcification is not a common finding and has been reported more frequently in the optic nerve, hypothalamic/thalamus and superficially located cerebral tumors. We present a cerebellar PA in a 3-year-old male patient with cystic components and massive calcification areas. The residual tumor grew rapidly after the first operation, and the patient was operated on again. A histopathological examination revealed polar spongioblastoma-like cells. Massive calcification is not a common feature in PAs and can lead to difficulties in radiological and pathological differential diagnoses.
MeSH Terms
Figure
-
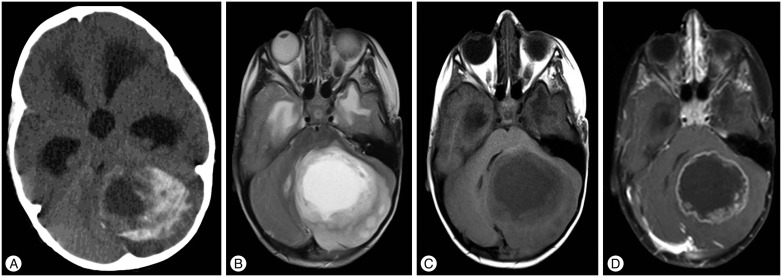
Fig. 1 Preoperative radiological findings. A : Preoperative CT demonstrated cystic, peripheral enhancing calcified lesion. B : Axial T2-weighted MRI demonstrated cystic heterogeneously mass with peripheral edema. C : Axial T1-weighted MRI demonstrated hypodense cystic mass. D : Post-contrast axial T1-weighted MRI demonstrated peripheral contrast enhancing mass.
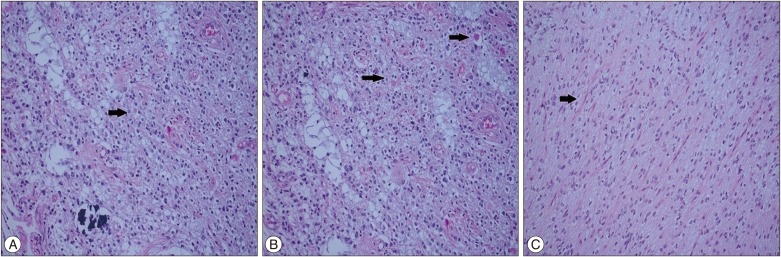
Fig. 2 Pathologic findings after first operation. A : Rare eosinophilic bodies reveal adjacent to calcification (arrow) (H&E ×200). B : Eosinophilic bodies and biphasic pilocytic areas (arrows) (H&E ×200). C : Rosenthal fibers and biphasic dense areas of the tumor (arrow) (H&E ×200).

Fig. 3 CTs and MRI showing residual calcified tumor growth. A : Post-operative CT on first day. B : Post-operative CT on 6-month. C : Post-operative CT on 12-month. D : There is no contrast enhancing area on the 6-month axial post-contrast T1-weighted MRI. E : T2-weighted MRI revealed cystic and heterogeneous appearance on the 12-month. F : Post-contrast T1-weighted MRI revealed prominent contrast-enhancing regions.

Fig. 4 Pathologic findings after second operation. A : Areas with palisading sequence and calcification (H&E ×200). B : Oligodendroglioma-like cells (H&E ×200).

Fig. 5 Tumor pathology was not detected after second operation. A : Axial CT. B : Axial T2-weighted MRI. C : Sagittal T1-weighted MRI.
Reference
-
1. Burger PC, Scheithauer BW, Paulus W, Szymas J, Giannini C, Kleihues P. Pilocytic astrocytoma. In : Kleihues P, Cavenee W, editors. Pathology and genetics of tumours of the nervous system. ed 2. Lyon, France: IARC;2000. p. 44–51.2. Fernandez C, Figarella-Branger D, Girard N, Bouvier-Labit C, Gouvernet J, Paz Paredes A, et al. Pilocytic astrocytomas in children : prognostic factors--a retrospective study of 80 cases. Neurosurgery. 2003; 53:544–553. PMID: 12943571.3. Friedman JH, Chiucchini I, Tucci JR. Idiopathic hypoparathyroidism with extensive brain calcification and persistent neurologic dysfunction. Neurology. 1987; 37:307–309. PMID: 3808313.
Article4. Fukushima S, Narita Y, Shinomiya A, Ohno M, Miyakita Y, Okita Y, et al. A case of unclassified high-grade glioma with polar spongioblastoma pattern. Neuropathology. 2012; 32:604–610. PMID: 22393945.
Article5. Gilbertson EL, Good CA. Roentgenographic signs of tumors of the brain. Am J Roentgenol Radium Ther Nucl Med. 1956; 76:226–247.6. Halpin S, Kingsley D. Disappearance of cerebral calcification as a sign of tumor growth. AJNR Am J Neuroradiol. 1993; 14:119–122. PMID: 8427072.7. Heideman RL, Packer RJ, Albright AL, Freeman CR, Rorke LB. Tumors of the Central Nervous System. In : Pizzo PA, Poplack DG, editors. Principles and Pediatric Oncology. ed 3. hiladelphia: Lipincott-Raven;1997. p. 663–697.8. Kalan C, Burrows EH. Calcification in intracranial gliomata. Br J Radiol. 1962; 35:589–602. PMID: 14453218.
Article9. Kim YE, Shin HJ, Suh YL. Pilocytic astrocytoma with extensive psammomatous calcification in the lateral ventricle : a case report. Childs Nerv Syst. 2012; 28:649–652. PMID: 22167267.
Article10. Koeller KK, Rushing EJ. From the archives of the AFIP : pilocytic astrocytoma : radiologic-pathologic correlation. Radiographics. 2004; 24:1693–1708. PMID: 15537977.11. Kumar R, Garg K, Kakkar A, Sharma MC. Giant calcified intraventricular pilocytic astrocytoma : a rare entity. Neurol India. 2014; 62:71–73. PMID: 24608462.
Article12. Okuchi K, Hiramatsu K, Morimoto T, Tsunoda S, Sakaki T, Iwasaki S. Astrocytoma with widespread calcification along axonal fibres. Neuroradiology. 1992; 34:328–330. PMID: 1528446.
Article13. Tihan T, Burger PC. A variant of “pilocytic astrocytoma” - a possible district clinicopathological entity with a less favorable outcome. J Neuropathol Exp Neurol. 1998; 57:500.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Multiple Solid Pilocytic Astrocytomas in Cerebellum with Neurofibromatosis Type I: A Case Report
- A Case of Huge Pilocytic Astrocytoma Causing Eyeball Subluxation
- Cerebellar Pilocytic Astrocytomas with Spontaneous Intratumoral Hemorrhage in Adult
- Neurofibromatosis Type 1 with Cerebellar Piloytic Astrocytoma
- Supratentorial Pilocytic Astrocytoma Mimicking Convexity Meningioma with Early Anaplastic Transformation: A Case Report
