Features of Undiagnosed Breast Cancers at Screening Breast MR Imaging and Potential Utility of Computer-Aided Evaluation
- Affiliations
-
- 1Department of Radiology, Seoul National University Hospital, Seoul 03080, Korea. river7774@gmail.com
- 2Department of Radiology, Chung-Ang University Hospital, Seoul 06973, Korea.
- 3Department of Radiology, Seoul National College of Medicine, Seoul 03080, Korea.
- 4Institute of Radiation Medicine, Seoul National University Medical Research Center, Seoul 03080, Korea.
- 5Department of Radiology, Hanyang University College of Medicine, Seoul 04763, Korea.
- 6Department of Radiology, SMG-SNU Boramae Medical Center, Seoul 07061, Korea.
- KMID: 2351164
- DOI: http://doi.org/10.3348/kjr.2016.17.1.59
Abstract
OBJECTIVE
To retrospectively evaluate the features of undiagnosed breast cancers on prior screening breast magnetic resonance (MR) images in patients who were subsequently diagnosed with breast cancer, as well as the potential utility of MR-computer-aided evaluation (CAE).
MATERIALS AND METHODS
Between March 2004 and May 2013, of the 72 consecutive pairs of prior negative MR images and subsequent MR images with diagnosed cancers (median interval, 32.8 months; range, 5.4-104.6 months), 36 (50%) had visible findings (mean size, 1.0 cm; range, 0.3-5.2 cm). The visible findings were divided into either actionable or underthreshold groups by the blinded review by 5 radiologists. MR imaging features, reasons for missed cancer, and MR-CAE features according to actionability were evaluated.
RESULTS
Of the 36 visible findings on prior MR images, 33.3% (12 of 36) of the lesions were determined to be actionable and 66.7% (24 of 36) were underthreshold; 85.7% (6 of 7) of masses and 31.6% (6 of 19) of non-mass enhancements were classified as actionable lesions. Mimicking physiologic enhancements (27.8%, 10 of 36) and small lesion size (27.8%, 10 of 36) were the most common reasons for missed cancer. Actionable findings tended to show more washout or plateau kinetic patterns on MR-CAE than underthreshold findings, as the 100% of actionable findings and 46.7% of underthreshold findings showed washout or plateau (p = 0.008).
CONCLUSION
MR-CAE has the potential for reducing the number of undiagnosed breast cancers on screening breast MR images, the majority of which are caused by mimicking physiologic enhancements or small lesion size.
MeSH Terms
Figure
-

Fig. 1 Screening breast MR images of 31-year-old woman with personal history of contralateral breast cancer. Breast MRI was reported as negative finding with severe background parenchymal enhancement. This case was classified as actionable and reason for undiagnosis was determined as severe background parenchymal enhancement. Pre-contrast (A), early post-contrast (B), and delayed post-contrast (C) phase sagittal MR images show focal heterogeneous non-mass enhancement in upper breast (arrows). D. Retrospectively applied MR-computer-aided evaluation image shows lesion displaying mixed red, yellow, and blue color codings indicative of washout kinetic pattern based on most suspicious feature (arrows). E. Seven months later, patient was diagnosed with 1.6 cm high-grade invasive ductal carcinoma. Diagnostic MR image shows irregular, rim-enhancing mass (arrow).
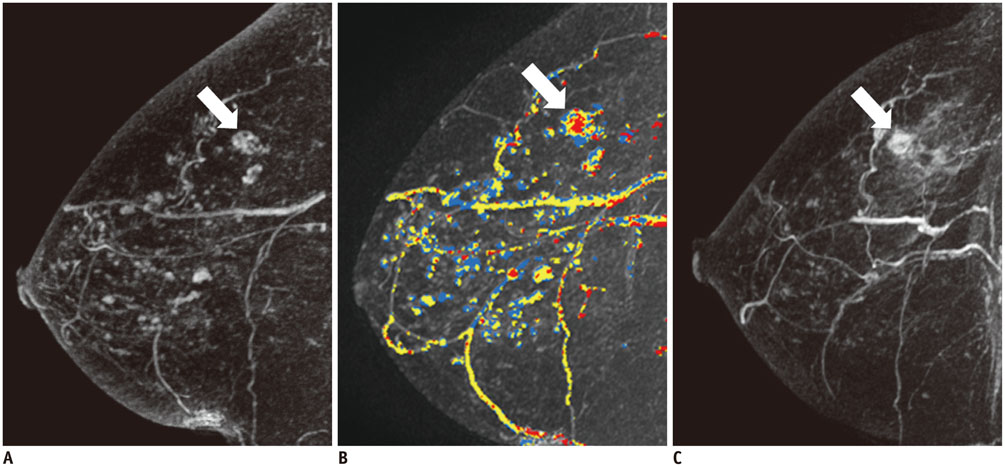
Fig. 2 Screening breast MR images of 46-year-old woman with personal history of contralateral breast cancer. Breast MRI was reported as multiple benign findings in both breasts. This case was classified as actionable and reason for missed cancer was determined as multiple distracting lesions. A. Three-dimensional maximum intensity projection image of early post-contrast phase, sagittal MR images show multiple enhancing foci and masses in breast (arrow). B. Retrospectively applied MR-computer-aided evaluation image shows lesion displaying mixed red, yellow, and blue color codings indicative of washout kinetic patterns based on most suspicious feature (arrow). C. Seven months later, she was diagnosed with 1.0 cm intermediate grade invasive ductal carcinoma. Diagnostic MR image shows irregular, heterogeneously enhancing mass (arrow).
Cited by 2 articles
-
Features of Pure Lobular Carcinoma In Situ on Magnetic Resonance Imaging Associated with Immediate Re-Excision after Lumpectomy
A Jung Chu, Nariya Cho, In-Ae Park, Seong Whi Cho
J Breast Cancer. 2016;19(2):199-205. doi: 10.4048/jbc.2016.19.2.199.Identification of Preoperative Magnetic Resonance Imaging Features Associated with Positive Resection Margins in Breast Cancer: A Retrospective Study
Jung-Hyun Kang, Ji Hyun Youk, Jeong-Ah Kim, Hye Mi Gweon, Na Lae Eun, Kyung Hee Ko, Eun Ju Son
Korean J Radiol. 2018;19(5):897-904. doi: 10.3348/kjr.2018.19.5.897.
Reference
-
1. Saslow D, Boetes C, Burke W, Harms S, Leach MO, Lehman CD, et al. American Cancer Society guidelines for breast screening with MRI as an adjunct to mammography. CA Cancer J Clin. 2007; 57:75–89.2. Kriege M, Brekelmans CT, Boetes C, Besnard PE, Zonderland HM, Obdeijn IM, et al. Efficacy of MRI and mammography for breast-cancer screening in women with a familial or genetic predisposition. N Engl J Med. 2004; 351:427–437.3. Kuhl CK, Schrading S, Leutner CC, Morakkabati-Spitz N, Wardelmann E, Fimmers R, et al. Mammography, breast ultrasound, and magnetic resonance imaging for surveillance of women at high familial risk for breast cancer. J Clin Oncol. 2005; 23:8469–8476.4. Warner E, Plewes DB, Hill KA, Causer PA, Zubovits JT, Jong RA, et al. Surveillance of BRCA1 and BRCA2 mutation carriers with magnetic resonance imaging, ultrasound, mammography, and clinical breast examination. JAMA. 2004; 292:1317–1325.5. Sardanelli F, Podo F, D'Agnolo G, Verdecchia A, Santaquilani M, Musumeci R, et al. Multicenter comparative multimodality surveillance of women at genetic-familial high risk for breast cancer (HIBCRIT study): interim results. Radiology. 2007; 242:698–715.6. Leach MO, Boggis CR, Dixon AK, Easton DF, Eeles RA, Evans DG, et al. Screening with magnetic resonance imaging and mammography of a UK population at high familial risk of breast cancer: a prospective multicentre cohort study (MARIBS). Lancet. 2005; 365:1769–1778.7. Kuhl CK, Schrading S, Bieling HB, Wardelmann E, Leutner CC, Koenig R, et al. MRI for diagnosis of pure ductal carcinoma in situ: a prospective observational study. Lancet. 2007; 370:485–492.8. Baur A, Bahrs SD, Speck S, Wietek BM, Krämer B, Vogel U, et al. Breast MRI of pure ductal carcinoma in situ: sensitivity of diagnosis and influence of lesion characteristics. Eur J Radiol. 2013; 82:1731–1737.9. Obdeijn IM, Loo CE, Rijnsburger AJ, Wasser MN, Bergers E, Kok T, et al. Assessment of false-negative cases of breast MR imaging in women with a familial or genetic predisposition. Breast Cancer Res Treat. 2010; 119:399–407.10. Pages EB, Millet I, Hoa D, Doyon FC, Taourel P. Undiagnosed breast cancer at MR imaging: analysis of causes. Radiology. 2012; 264:40–50.11. Birdwell RL, Ikeda DM, O'Shaughnessy KF, Sickles EA. Mammographic characteristics of 115 missed cancers later detected with screening mammography and the potential utility of computer-aided detection. Radiology. 2001; 219:192–202.12. Ikeda DM, Birdwell RL, O'Shaughnessy KF, Sickles EA, Brenner RJ. Computer-aided detection output on 172 subtle findings on normal mammograms previously obtained in women with breast cancer detected at follow-up screening mammography. Radiology. 2004; 230:811–819.13. Williams TC, DeMartini WB, Partridge SC, Peacock S, Lehman CD. Breast MR imaging: computer-aided evaluation program for discriminating benign from malignant lesions. Radiology. 2007; 244:94–103.14. Wang LC, DeMartini WB, Partridge SC, Peacock S, Lehman CD. MRI-detected suspicious breast lesions: predictive values of kinetic features measured by computer-aided evaluation. AJR Am J Roentgenol. 2009; 193:826–831.15. Yamaguchi K, Schacht D, Newstead GM, Bradbury AR, Verp MS, Olopade OI, et al. Breast cancer detected on an incident (second or subsequent) round of screening MRI: MRI features of false-negative cases. AJR Am J Roentgenol. 2013; 201:1155–1163.16. Morris EA, Comstock CE, Lee CH. ACR BI-RADS® Magnetic Resonance Imaging. ACR BI-RADS® Atlas, Breast Imaging Reporting and Data System. Reston, VA: American College of Radiology;2013.17. Mahoney MC, Gatsonis C, Hanna L, DeMartini WB, Lehman C. Positive predictive value of BI-RADS MR imaging. Radiology. 2012; 264:51–58.18. DeMartini WB, Liu F, Peacock S, Eby PR, Gutierrez RL, Lehman CD. Background parenchymal enhancement on breast MRI: impact on diagnostic performance. AJR Am J Roentgenol. 2012; 198:W373–W380.19. Hambly NM, Liberman L, Dershaw DD, Brennan S, Morris EA. Background parenchymal enhancement on baseline screening breast MRI: impact on biopsy rate and short-interval follow-up. AJR Am J Roentgenol. 2011; 196:218–224.20. Lehman CD, Blume JD, DeMartini WB, Hylton NM, Herman B, Schnall MD. Accuracy and interpretation time of computer-aided detection among novice and experienced breast MRI readers. AJR Am J Roentgenol. 2013; 200:W683–W689.21. Cho N, Kim SM, Park JS, Jang M, Kim SY, Chang JM, et al. Contralateral lesions detected by preoperative MRI in patients with recently diagnosed breast cancer: application of MR CAD in differentiation of benign and malignant lesions. Eur J Radiol. 2012; 81:1520–1526.22. Su MY, Cheung YC, Fruehauf JP, Yu H, Nalcioglu O, Mechetner E, et al. Correlation of dynamic contrast enhancement MRI parameters with microvessel density and VEGF for assessment of angiogenesis in breast cancer. J Magn Reson Imaging. 2003; 18:467–477.23. Lee SH, Cho N, Kim SJ, Cha JH, Cho KS, Ko ES, et al. Correlation between high resolution dynamic MR features and prognostic factors in breast cancer. Korean J Radiol. 2008; 9:10–18.24. Liu YH, Xu L, Liu LH, Liu XS, Hou ZY, Hou DL, et al. 3.0T MR-CAD: Clinical Value in Diagnosis of Breast Tumor Compared with Conventional MRI. J Cancer. 2014; 5:585–589.25. Teifke A, Hlawatsch A, Beier T, Werner Vomweg T, Schadmand S, Schmidt M, et al. Undetected malignancies of the breast: dynamic contrast-enhanced MR imaging at 1.0 T. Radiology. 2002; 224:881–888.26. Soderstrom CE, Harms SE, Farrell RS Jr, Pruneda JM, Flamig DP. Detection with MR imaging of residual tumor in the breast soon after surgery. AJR Am J Roentgenol. 1997; 168:485–488.27. Belli P, Costantini M, Romani M, Marano P, Pastore G. Magnetic resonance imaging in breast cancer recurrence. Breast Cancer Res Treat. 2002; 73:223–235.
