Effect of Reducing Abdominal Compression during Prone CT Colonography on Ascending Colonic Rotation during Supine-to-Prone Positional Change
- Affiliations
-
- 1Department of Radiology and Research Institute of Radiology, University of Ulsan College of Medicine, Asan Medical Center, Seoul 05505, Korea. parksh.radiology@gmail.com
- KMID: 2351162
- DOI: http://doi.org/10.3348/kjr.2016.17.1.47
Abstract
OBJECTIVE
To determine the effect of reduced abdominal compression in prone position on ascending colonic movement during supine-to-prone positional change during CT colonography (CTC).
MATERIALS AND METHODS
Eighteen consecutive patients who had undergone prone CTC scanning with cushion blocks placed under the chest and hip/thigh to reduce abdominal compression and had confirmed sessile polyps > or = 6 mm in the well-distended, straight, mid-ascending colon, were included. Radial location along the ascending colonic luminal circumference (degrees) was measured for 24 polyps and 54 colonic teniae on supine and prone CTC images. The supine-to-prone change ranging between -180degrees and +180degrees (- and + for internal and external colonic rotations, respectively), was determined. In addition, possible causes of any ascending colonic rotations were explored.
RESULTS
Abdominal compression during prone CTC scanning completely disappeared with the use of cushion blocks in 17 of 18 patients. However, some degrees of ascending colonic rotation were still observed, with the radial location changes of -22degrees to 61degrees (median, 13.9degrees) for the polyps and similar degrees for teniae. Fifty-four percent and 56% of polyps and teniae, respectively, showed changes > 10degrees. The radial location change of the polyps was significantly associated with the degree of anterior shift of the small bowel and mesentery (r = 0.722, p < 0.001) and the degree of posterior displacement of the ascending colon (r = 0.566, p = 0.004) during supine-to-prone positional change.
CONCLUSION
Ascending colonic rotation upon supine-to-prone positional change during CTC, mostly in the form of external rotation, is not eliminated by removing abdominal compression in prone position.
MeSH Terms
Figure
-
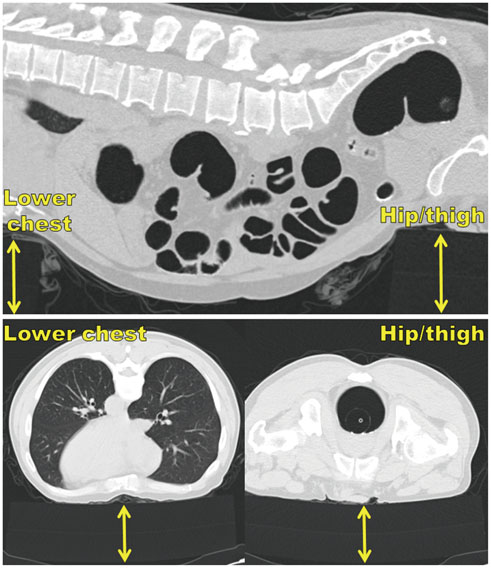
Fig. 1 Placement of 2 cushion blocks (double arrows) under lower chest and hip/thigh in prone position demonstrated in sagittal (upper) and transverse (lower) images.

Fig. 2 Coordinate system to determine radial location of polyp or tenia along circumference of mid-ascending colon in supine (A) and prone (B) positions. Horizontal, white line (labeled as A) is drawn to connect lateral tips of transverse processes of lumbar vertebra that are closest to polyp of interest (which is projected onto present image at exact level where polyp is shown) and is used as reference horizontal line. Blue line (labeled as B) parallel to line A is drawn to pass through center of distended, mid-ascending colonic lumen. 2 points where line B meets with colon wall are given circumferential coordinates of 90° and 270°. Another green line (labeled as C) that is perpendicular to line B and passes through center of ascending colonic lumen is drawn. 2 points where this line crosses colon wall are designated as 0° and 180°. Radial location of polyp (arrows) is then obtained by measuring angle between vertical line of 0° and line that connects center of lumen and center of polyp in degrees with clockwise increments. Polyp radial location in this example is 243° and 226° in supine and prone positions, respectively, indicating external rotation of ascending colon by 17° during supine-to-prone position change.

Fig. 3 Measurement of anthropometric indices. Abdcomp is defined as (abdominal thicknesssupine - abdominal thicknessprone) / abdominal thicknesssupine x 100%, where abdominal thickness was distance from anterior abdominal wall to anterior margin of lumbar spine at level of umbilicus. Ascdisp, distance of ascending colonic movement in anteroposterior direction vertical to aforementioned reference horizontal line, is calculated by comparing distance labeled as d, vertical anteroposterior distance between horizontal line that passes through center of distended mid-ascending colon, and parallel horizontal line that is tangent to anterior margin of lumbar spine, between supine and prone positions.
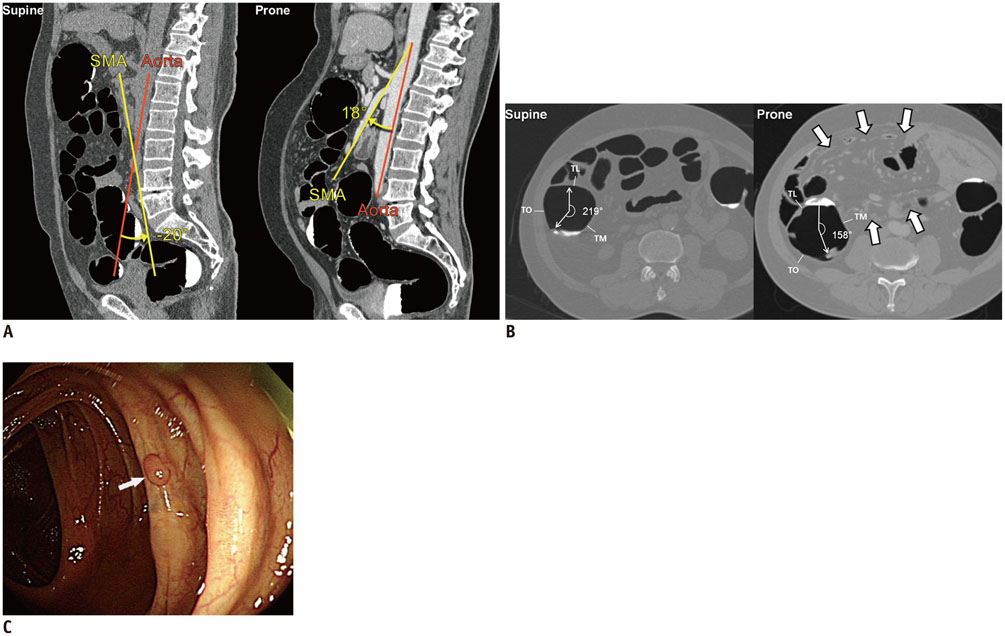
Fig. 4 Anterior displacement of mesentery and small bowel, which pushes ascending colon posterolaterally in 59-year-old man. A. SMAshift measured by difference in aorto-mesenteric angle, which is angle between abdominal aorta (Aorta; red line) and straight main trunk of superior mesenteric artery (SMA; yellow line), between prone and supine positions is 38° in this example, i.e., prone angle of 18° - supine angle of -20°. B. External rotation of ascending colon by 61° (219° - 158°) during supine-to-prone positional change in absence of abdominal compression is demonstrated by radial locations of 6-mm, sessile, tubular adenoma. Prone CT colonography image shows large lump consisting of mesentery and small bowel, which is displaced anteriorly due to gravity and occupying large space in anteromedial side of abdomen (arrows). TM, TL, and TO represent tenia mesocolica, tenia libera, and tenia omentalis. C. Endoscopic image shows sessile polyp (arrow) in mid-ascending colon.
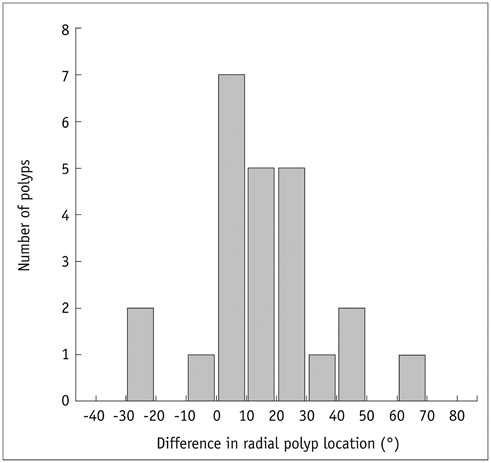
Fig. 5 Histogram showing distribution of polyp radial location difference during supine-to-prone positional change. Each bar represents number of polyps for each 10° range, e.g., 7 polyps in 0° to < 10° range. Negative and positive values (°) represent internal and external rotation, respectively, of ascending colon in prone position, as compared with supine position.
Reference
-
1. Dachman AH. Scheduling, performing and reporting CT colonography. In : Dachman AH, Laghi A, editors. Atlas of virtual colonoscopy. 2nd ed. New York, NY: Springer-Verlag, Inc.;2011. p. 87–109.2. Kim DH, Pickhardt PJ. MDCT protocol for CT colonography. In : Pickhardt PJ, Kim DH, editors. CT colonography: principles and practice of virtual colonoscopy. 1st ed. Philadelphia, PA: Saunders Elsevier;2010. p. 148–156.3. Neri E, Halligan S, Hellström M, Lefere P, Mang T, Regge D, et al. The second ESGAR consensus statement on CT colonography. Eur Radiol. 2013; 23:720–729.4. Chen SC, Lu DS, Hecht JR, Kadell BM. CT colonography: value of scanning in both the supine and prone positions. AJR Am J Roentgenol. 1999; 172:595–599.5. Fletcher JG, Johnson CD, Welch TJ, MacCarty RL, Ahlquist DA, Reed JE, et al. Optimization of CT colonography technique: prospective trial in 180 patients. Radiology. 2000; 216:704–711.6. Morrin MM, Farrell RJ, Keogan MT, Kruskal JB, Yam CS, Raptopoulos V. CT colonography: colonic distention improved by dual positioning but not intravenous glucagon. Eur Radiol. 2002; 12:525–530.7. Yee J, Kumar NN, Hung RK, Akerkar GA, Kumar PR, Wall SD. Comparison of supine and prone scanning separately and in combination at CT colonography. Radiology. 2003; 226:653–661.8. Boone DJ, Halligan S, Roth HR, Hampshire TE, Helbren E, Slabaugh GG, et al. CT colonography: external clinical validation of an algorithm for computer-assisted prone and supine registration. Radiology. 2013; 268:752–760.9. Punwani S, Halligan S, Tolan D, Taylor SA, Hawkes D. Quantitative assessment of colonic movement between prone and supine patient positions during CT colonography. Br J Radiol. 2009; 82:475–481.10. Chen JC, Dachman AH. Cecal mobility: a potential pitfall of CT colonography. AJR Am J Roentgenol. 2006; 186:1086–1089.11. Mang T, Maier A, Plank C, Mueller-Mang C, Herold C, Schima W. Pitfalls in multi-detector row CT colonography: a systematic approach. Radiographics. 2007; 27:431–454.12. Kim JY, Park SH, Lee SS, Kim AY, Ha HK. Ascending colon rotation following patient positional change during CT colonography: a potential pitfall in interpretation. Eur Radiol. 2011; 21:353–359.13. Saunders BP, Phillips RK, Williams CB. Intraoperative measurement of colonic anatomy and attachments with relevance to colonoscopy. Br J Surg. 1995; 82:1491–1493.14. Saunders BP, Masaki T, Sawada T, Halligan S, Phillips RK, Muto T, et al. A peroperative comparison of Western and Oriental colonic anatomy and mesenteric attachments. Int J Colorectal Dis. 1995; 10:216–221.15. Lee SS, Park SH, Kim JK, Kim N, Lee J, Park BJ, et al. Panoramic endoluminal display with minimal image distortion using circumferential radial ray-casting for primary three-dimensional interpretation of CT colonography. Eur Radiol. 2009; 19:1951–1959.16. Buchach CM, Kim DH, Pickhardt PJ. Performing an additional decubitus series at CT colonography. Abdom Imaging. 2011; 36:538–544.17. Gryspeerdt SS, Herman MJ, Baekelandt MA, van Holsbeeck BG, Lefere PA. Supine/left decubitus scanning: a valuable alternative to supine/prone scanning in CT colonography. Eur Radiol. 2004; 14:768–777.18. Pickhardt PJ, Bakke J, Kuo J, Robbins JB, Lubner MG, del Rio AM, et al. Volumetric analysis of colonic distention according to patient position at CT colonography: diagnostic value of the right lateral decubitus series. AJR Am J Roentgenol. 2014; 203:W623–W628.19. Lee JH, Park SH, Lee SS, Kim AY, Kim JC, Yu CS, et al. CT colonography in patients who have undergone sigmoid colostomy: a feasibility study. AJR Am J Roentgenol. 2011; 197:W653–W657.20. Culligan K, Coffey JC, Kiran RP, Kalady M, Lavery IC, Remzi FH. The mesocolon: a prospective observational study. Colorectal Dis. 2012; 14:421–428. discussion 428-430
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Change in Intraocular Pressure According to Sleeping Posture in Normal People
- The changes of endotracheal tube cuff pressure by the position changes from supine to prone and the flexion and extension of head
- The Diagnostic Utility of Prone Position Chest CT for the Evaluation of Esophageal Cancer
- The Comparison of Sleep Characteristics According to the Sleep Positions in Healthy Newborns
- CT Arthrographic Finding in Shoulder Instability
