The Diagnostic Utility of Prone Position Chest CT for the Evaluation of Esophageal Cancer
- Affiliations
-
- 1Department of Radiology, Chonnam National University Hospital, Gwangju, Korea. yhkim001@jnu.ac.kr
- 2Department of Radiology, Chonnam National University Medical School, Gwangju, Korea.
- 3Department of Cardiothoracic Surgery, Chonnam National University Medical School, Gwangju, Korea.
- KMID: 2468149
- DOI: http://doi.org/10.4068/cmj.2020.56.1.68
Abstract
- The aim of this study was to assess the potential of a prone chest CT for the evaluation of esophageal cancer, as compared with a routine supine chest CT. 69 patients (67±18 years old) with pathologically confirmed esophageal cancers underwent MDCT in the supine and prone positions. The supine CT was performed first, followed by the prone position. Localization and staging of individual esophageal lesions on both the prone and supine CTs were assessed by two thoracic radiologists, using a scoring system that consisted of three confidence scales, and the results were correlated with the endoscopic and surgical findings. The mean confidence score for the detection of esophageal cancer was higher in the prone position (2.58±0.74) than that in the supine position (2.42±0.83) with statistical significance (p=0.002). The mean confidence score for predicting local invasion in the selected patients (n=18) who underwent esophagectomy was also higher in the prone position (2.39±0.85) than that in the supine position (2.06±0.73) with statistical significance (p=0.01). In 10 of 11 cases that showed definitive determination for periesophageal infiltration or adjacent organ invasion on the prone CT (score 3), the corresponding findings were also observed in the post-operative evaluations. In conclusion, prone chest CT for evaluating esophageal cancer could have advantages in regards to the localization of esophageal cancer and predicting local invasion compared to that of routine supine CT and can improve the diagnostic accuracy of chest CTs.
Keyword
MeSH Terms
Figure
-
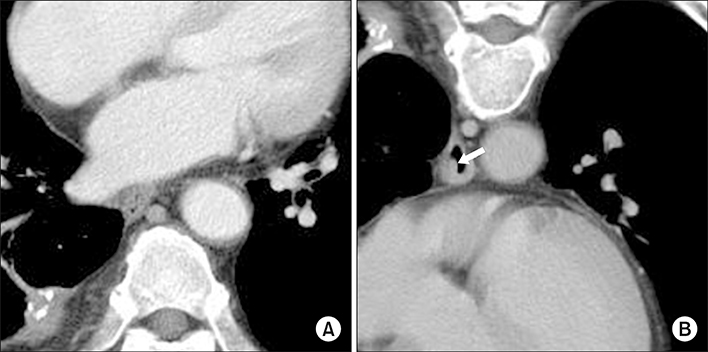
FIG. 1 A 75-year-old man with squamous cell carcinoma in the distal esophagus. (A) The axial contrast-enhanced CT scan with the patient in the supine position shows a collapsed esophageal lumen without any detectable mass-like lesion. (B) The axial contrast-enhanced CT scan with the patient in the prone position demonstrates eccentric nodular wall thickening (arrow) by virtue of the broaden interspace between the heart and vertebra and the distended esophagus.

FIG. 2 A 61-year-old man with squamous cell carcinoma in the mid esophagus. (A and B) The axial contrast enhanced CT scans (A and B) show a protruding mass (black arrows in A and B) in the esophagus. The axial CT scan with the patient in the supine position (A) demonstrates the esophagus, which abuts against the thoracic aorta (arrowheads), with suspicious invasion. However, the axial CT scan with the patient in the prone position (B) clearly demonstrates a fat plane (arrowheads) between the esophageal tumor and thoracic aorta, without evidence of invasion. Esophagectomy was performed in this patient and the postoperative TNM stage was determined to be T2 N0 M0.

FIG. 3 A 72-year-old man with mid esophageal cancer. (A) The axial contrast-enhanced CT scan with the patient in the supine position shows a hypo-attenuation lesion (white arrow) in the distal esophagus. (B) The axial contrast-enhanced CT scan with the patient in the prone position clearly shows the presence of hypo-attenuation lesion (white arrow in A) that is a necrotizing metastatic lymph node (arrowheads) rather than an esophageal lesion by virtue of the broaden interspace between the esophagus and the vertebral body.
Reference
-
1. Panebianco V, Grazhdani H, Iafrate F, Petroni M, Anzidei M, Laghi A, et al. 3D CT protocol in the assessment of the esophageal neoplastic lesions: can it improve TNM staging? Eur Radiol. 2006; 16:414–421.
Article2. Umeoka S, Koyama T, Togashi K, Saga T, Watanabe G, Shimada Y, et al. Esophageal cancer: evaluation with triple-phase dynamic CT--initial experience. Radiology. 2006; 239:777–783.
Article3. Ba-Ssalamah A, Zacherl J, Noebauer-Huhmann IM, Uffmann M, Matzek WK, Pinker K, et al. Dedicated multi-detector CT of the esophagus: spectrum of diseases. Abdom Imaging. 2009; 34:3–18.
Article4. Kim SH, Lee JM, Han JK, Kim YH, Lee JY, Lee HJ, et al. Three-dimensional MDCT imaging and CT esophagography for evaluation of esophageal tumors: preliminary study. Eur Radiol. 2006; 16:2418–2426.
Article5. Agrawal B. CT findings in patients with esophageal carcinoma and its correlation with esophagographic findings. Open J Radiol. 2018; 8:109–124.
Article6. Faigel DO. The role of endoscopic ultrasound in esophageal cancer. Gastroenterol Hepatol (N Y). 2019; 15:519–521.7. Luo LN, He LJ, Gao XY, Huang XX, Shan HB, Luo GY, et al. Evaluation of preoperative staging for esophageal squamous cell carcinoma. World J Gastroenterol. 2016; 22:6683–6689.
Article8. van den Hoed RD, Feldberg MA, van Leeuwen MS, van Dalen T, Obertop H, Kooyman CD, et al. CT prediction of irresectability in esophageal carcinoma: value of additional patient positions and relation to patient outcome. Abdom Imaging. 1997; 22:132–137.
Article9. Wayman J, Chakraverty S, Griffin SM, Doyle GJ, Keir MJ, Simpson W. Evaluation of local invasion by oesophageal carcinoma--a prospective study of prone computed tomography scanning. Postgrad Med J. 2001; 77:181–184.
Article10. Helmberger H. CT for local staging of esophageal cancer. Dis Esophagus. 1999; 12:202–204.
Article11. Yamabe Y, Kuroki Y, Ishikawa T, Miyakawa K, Kuroki S, Sekiguchi R. Tumor staging of advanced esophageal cancer: combination of double-contrast esophagography and contrast-enhanced CT. AJR Am J Roentgenol. 2008; 191:753–757.
Article12. Zhou SL, Zhou XY, Liu XJ, Bo GJ, Gu Y, Chen W. Comparison of dual source computed tomography (CT) and diffusion-weighted magnetic resonance imaging (MRI) for pathological classification of esophageal cancer. Int J Clin Exp Med. 2018; 11:12578–12584.13. Pongpornsup S, Posri S, Totanarungroj K. Diagnostic accuracy of multidetector computed tomography (MDCT) in evaluation for mediastinal invasion of esophageal cancer. J Med Assoc Thai. 2012; 95:704–711.14. Legmann P, Marmuse JP, Rjob S, Benacerraf R. Preoperative computed tomography for transhiatal esophagectomy. Invest Radiol. 1991; 26:987–991.
Article15. Maerz LL, Deveney CW, Lopez RR, McConnell DB. Role of computed tomographic scans in the staging of esophageal and proximal gastric malignancies. Am J Surg. 1993; 165:558–560.
Article16. Yoon YC, Lee KS, Shim YM, Kim BT, Kim K, Kim TS. Metastasis to regional lymph nodes in patients with esophageal squamous cell carcinoma: CT versus FDG PET for presurgical detection prospective study. Radiology. 2003; 227:764–770.
Article17. Ball WS, Wicks JD, Mettler FA Jr. Prone-supine change in organ position: CT demonstration. AJR Am J Roentgenol. 1980; 135:815–820.
Article18. Kim SH, Lee JM, Han JK, Lee JY, Yang HK, Lee HJ, et al. Effect of adjusted positioning on gastric distention and fluid distribution during CT gastrography. AJR Am J Roentgenol. 2005; 185:1180–1184.
Article19. Chen SC, Lu DS, Hecht JR, Kadell BM. CT colonography: value of scanning in both the supine and prone positions. AJR Am J Roentgenol. 1999; 172:595–599.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Video-Assisted Thoracic Surgery Esophagectomy
- Evaluation of Tumor Invasion in Gastric Carcinoma with CT Using Water as an Oral Contrast Agent in Prone Position
- The Effect of Prone Position on Pulmonary Compliances by Anesthesia Duration
- The Utility of Chest CTinStagingof Esophageal Cancer
- Extralevator Abdominoperineal Resection in the Prone Position
