Transvenous Lead Extraction via the Inferior Approach Using a Gooseneck Snare versus Simple Manual Traction
- Affiliations
-
- 1Heart Institute, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. mdjunkim@gmail.com
- 2Division of Cardiology, Department of Internal Medicine, Soonchunhyang University Hospital, Soonchunhyang University College of Medicine, Bucheon, Korea.
- 3Department of Radiology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- KMID: 2344470
- DOI: http://doi.org/10.4070/kcj.2016.46.2.186
Abstract
- BACKGROUND AND OBJECTIVES
The number of patients with cardiac implantable electronic devices needing lead extraction is increasing for various reasons, including infections, vascular obstruction, and lead failure. We report our experience with transvenous extraction of pacemaker and defibrillator leads via the inferior approach of using a gooseneck snare as a first-line therapy and compare extraction using a gooseneck snare with extraction using simple manual traction.
SUBJECTS AND METHODS
The study included 23 consecutive patients (43 leads) who underwent transvenous lead extraction using a gooseneck snare (group A) and 10 consecutive patients (17 leads) who underwent lead extraction using simple manual traction (group B). Patient characteristics, indications, and outcomes were analyzed and compared between the groups.
RESULTS
The dwelling time of the leads was longer in group A (median, 121) than in group B (median, 56; p=0.000). No differences were noted in the overall procedural success rate (69.6% vs. 70%), clinical procedural success rate (82.6% vs. 90%), and lead clinical success rate (86% vs. 94.1%) between the groups. The procedural success rates according to lead type were 89.2% and 100% for pacing leads and 66.7% and 83.3% for defibrillator leads in groups A and B, respectively. Major complications were noted in 3 (mortality in 1) patients in group A and 2 patients in group B.
CONCLUSION
Transvenous extraction of pacemaker leads via an inferior approach using a gooseneck snare was both safe and effective. However, stand-alone transvenous extraction of defibrillator leads using the inferior approach was suboptimal.
MeSH Terms
Figure
-
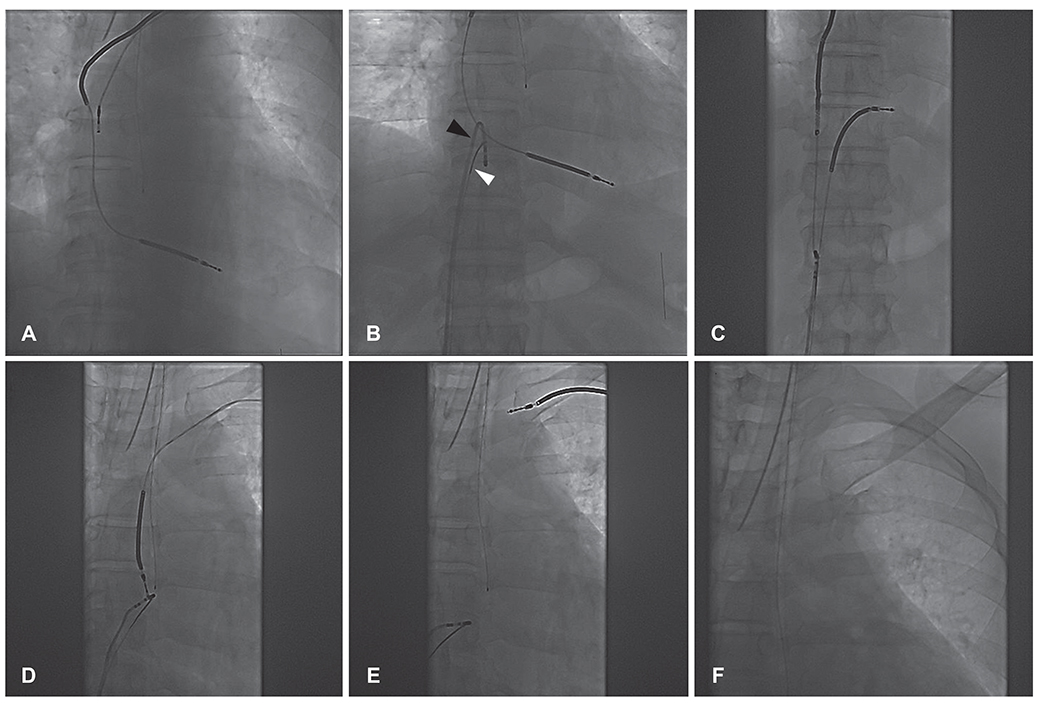
Fig. 1 Extraction of dual-chamber defibrillator leads. (A) The active fixation lead is removed by simple traction. (B) A closed loop is formed with the snare (white arrowhead) and ablation catheter (black arrowhead) capturing target ICD lead. (C) Downward traction of the snare and ablation catheter complex is performed gently. Repeated traction and release are required for complete removal. (D) The tip of the ICD lead is detached from the RV apex. The SVC coil is already moved into the subclavian vein with traction. (E) The entire ICD lead is removed by manual traction via the entry site. (F) Fluoroscopy shows absence of residual lead material. ICD: implantable cardioverter defibrillator, RV: right ventricle, SVC: superior vena cava.
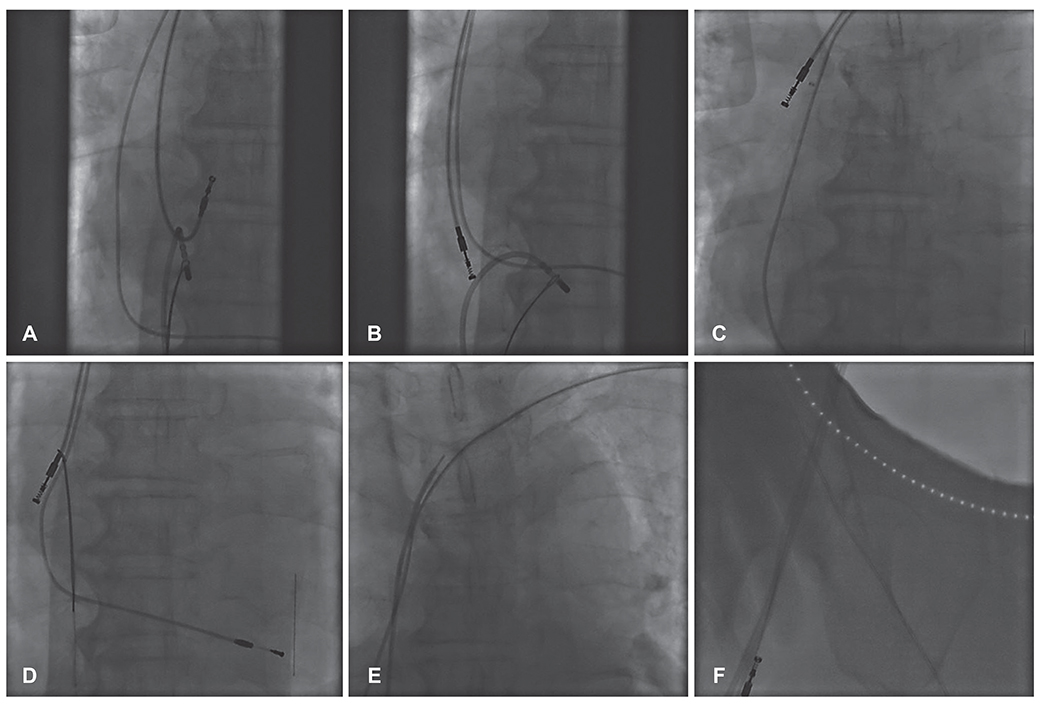
Fig. 2 Extraction of dual-chamber pacemaker leads. (A) The tip of ablation catheter is bended to anchor the right atrial lead. (B) A closed loop capturing target lead is formed with the snare and ablation catheter. (C) The right atrial lead is detached from the insertion site by gentle traction. (D) Manual removal of the detached right atrial lead via the entry site is impossible, probably due to venous occlusion. (E) The tip of the right atrial lead is grasped by the snare. (F) The lead is cut at the entry site. The proximal fragment was removed via entry site, and the distal fragment was removed easily via the femoral vein without residual lead material.
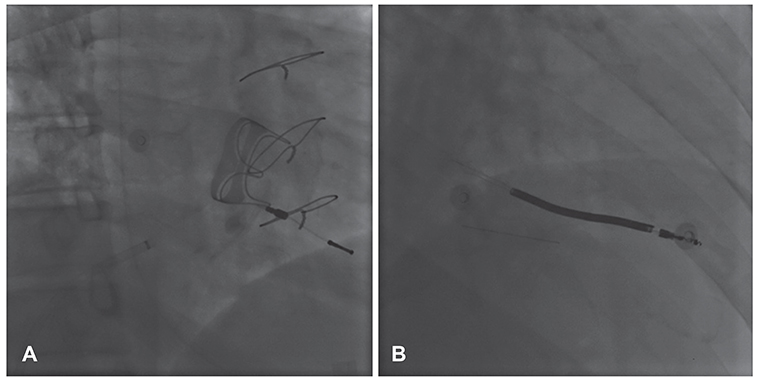
Fig. 3 Right anterior oblique views of the leads that could not be extracted via the femoral approach. (A) A remnant pacing lead in the right ventricle after surgical extraction could not be extracted owing to failure to capture the remnant lead. (B) A remnant defibrillator lead that was fractured during traction from below could not be removed owing to failure to capture the remnant lead.
Reference
-
1. Mond HG, Proclemer A. The 11th world survey of cardiac pacing and implantable cardioverter-defibrillators: calendar year 2009--a World Society of Arrhythmia's project. Pacing Clin Electrophysiol. 2011; 34:1013–1027.2. Greenspon AJ, Patel JD, Lau E, et al. 16-year trends in the infection burden for pacemakers and implantable cardioverter-defibrillators in the United States: 1993 to 2008. J Am Coll Cardiol. 2011; 58:1001–1006.3. Byrd CL, Schwartz SJ, Hedin NB, Goode LB, Fearnot NE, Smith HJ. Intravascular lead extraction using locking stylets and sheaths. Pacing Clin Electrophysiol. 1990; 13(12 Pt 2):1871–1875.4. Smith HJ, Fearnot NE, Byrd CL, Wilkoff BL, Love CJ, Sellers TD. Five-years experience with intravascular lead extraction. U.S. Lead Extraction Database. Pacing Clin Electrophysiol. 1994; 17(11 Pt 2):2016–2020.5. Wazni O, Epstein LM, Carrillo RG, et al. Lead extraction in the contemporary setting: the LExICon study: an observational retrospective study of consecutive laser lead extractions. J Am Coll Cardiol. 2010; 55:579–586.6. Neuzil P, Taborsky M, Rezek Z, et al. Pacemaker and ICD lead extraction with electrosurgical dissection sheaths and standard transvenous extraction systems: results of a randomized trial. Europace. 2007; 9:98–104.7. Wilkoff BL, Love CJ, Byrd CL, et al. Transvenous lead extraction: Heart Rhythm Society expert consensus on facilities, training, indications, and patient management: this document was endorsed by the American Heart Association (AHA). Heart Rhythm. 2009; 6:1085–1104.8. Yedlicka JW Jr, Carlson JE, Hunter DW, Castañeda-Zúñiga WR, Amplatz K. Nitinol gooseneck snare for removal of foreign bodies: experimental study and clinical evaluation. Radiology. 1991; 178:691–693.9. Dotter CT, Rösch J, Bilbao MK. Transluminal extraction of catheter and guide fragments from the heart and great vessels; 29 collected cases. Am J Roentgenol Radium Ther Nucl Med. 1971; 111:467–472.10. Bongiorni MG, Soldati E, Zucchelli G, et al. Transvenous removal of pacing and implantable cardiac defibrillating leads using single sheath mechanical dilatation and multiple venous approaches: high success rate and safety in more than 2000 leads. Eur Heart J. 2008; 29:2886–2893.11. Zhou X, Jiang H, Ma J, et al. Comparison of standard and modified transvenous techniques for complex pacemaker lead extractions in the context of cardiac implantable electronic device-related infections: a 10-year experience. Europace. 2013; 15:1629–1635.12. Jarwe M, Klug D, Beregi JP, et al. Single center experience with femoral extraction of permanent endocardial pacing leads. Pacing Clin Electrophysiol. 1999; 22:1202–1209.13. Klug D, Jarwé M, Messaoudéne SA, et al. Pacemaker lead extraction with the needle's eye snare for countertraction via a femoral approach. Pacing Clin Electrophysiol. 2002; 25:1023–1028.14. Belott PH. Lead extraction using the femoral vein. Heart Rhythm. 2007; 4:1102–1107.15. Hauser RG, Kallinen LM, Almquist AK, Gornick CC, Katsiyiannis WT. Early failure of a small-diameter high-voltage implantable cardioverter-defibrillator lead. Heart Rhythm. 2007; 4:892–896.16. Hauser RG, McGriff D, Retel LK. Riata implantable cardioverter-defibrillator lead failure: analysis of explanted leads with a unique insulation defect. Heart Rhythm. 2012; 9:742–749.17. Choi K, Kim JH, Kim HJ, Lee SO, Jang EY, Kim JS. A case of riata® dual coil defibrillator lead failure in a patient with ventricular fibrillation. Korean Circ J. 2013; 43:336–339.18. Maytin M, Love CJ, Fischer A, et al. Multicenter experience with extraction of the Sprint Fidelis implantable cardioverter-defibrillator lead. J Am Coll Cardiol. 2010; 56:646–650.19. Brunner MP, Cronin EM, Duarte VE, et al. Clinical predictors of adverse patient outcomes in an experience of more than 5000 chronic endovascular pacemaker and defibrillator lead extractions. Heart Rhythm. 2014; 11:799–805.20. Gomes S, Cranney G, Bennett M, Li A, Giles R. Twenty-year experience of transvenous lead extraction at a single centre. Europace. 2014; 16:1350–1355.21. Kennergren C, Bjurman C, Wiklund R, Gäbel J. A single-centre experience of over one thousand lead extractions. Europace. 2009; 11:612–617.22. Epstein AE, Kay GN, Plumb VJ, Dailey SM, Anderson PG. Gross and microscopic pathological changes associated with nonthoracotomy implantable defibrillator leads. Circulation. 1998; 98:1517–1524.23. Segreti L, Di Cori A, Soldati E, et al. Major predictors of fibrous adherences in transvenous implantable cardioverter-defibrillator lead extraction. Heart Rhythm. 2014; 11:2196–2201.24. Bordachar P, Defaye P, Peyrouse E, et al. Extraction of old pacemaker or cardioverter-defibrillator leads by laser sheath versus femoral approach. Circ Arrhythm Electrophysiol. 2010; 3:319–323.25. de Bie MK, Fouad DA, Borleffs CJ, et al. Trans-venous lead removal without the use of extraction sheaths, results of >250 removal procedures. Europace. 2012; 14:112–116.26. Epstein LM, Love CJ, Wilkoff BL, et al. Superior vena cava defibrillator coils make transvenous lead extraction more challenging and riskier. J Am Coll Cardiol. 2013; 61:987–989.27. Aoukar PS, Poole JE, Johnson GW, et al. No benefit of a dual coil over a single coil ICD lead: Evidence from the Sudden Cardiac Death in Heart Failure Trial. Heart Rhythm. 2013; 10:970–976.28. Kutyifa V, Huth Ruwald A-C, Aktas MK, et al. Clinical impact, safety, and efficacy of single- versus dual-coil ICD leads in MADIT-CRT. J Cardiovasc Electrophysiol. 2013; 24:1246–1252.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Removal of Entrapped Pacemaker Electrode: One Case Report
- Transvenous Lead Extraction
- Adjustment of Malpositioned Woven EndoBridge Device Using Gooseneck Snare: Complication Management Technique
- Successful Retrieval of Intravascular Stent Remnants With a Combination of Rotational Atherectomy and a Gooseneck Snare
- Implantable Cardioverter-Defibrillator Lead Extraction by Conventional Traction and Counter-Traction Technique
