A Case of the Third, Fourth, and Sixth Nerve Palsy in a Patient with Cerebral Aspergillosis
- Affiliations
-
- 1Department of Ophthalmology, Haeundae Paik Hospital, Inje University College of Medicine, Busan, Korea. Kris9352@hanmail.net
- KMID: 2339059
- DOI: http://doi.org/10.3341/jkos.2015.56.3.471
Abstract
- PURPOSE
To report a case of cerebral aspergillosis with third, fourth, and sixth nerve palsy.
CASE SUMMARY
A 66-year-old female presented with ocular pain, diplopia, ptosis, and limited ocular movement of the right eye. The patient had experienced rhinorrhea and headache in the right temporal area 3 weeks prior and was treated with oral antibiotics for 1 week. Marginal reflex distance 1 was -4 mm in the right eye and +4 mm in the left eye. Upward, downward, medial, and lateral gaze limitation (-4/-4/-3.5/-2.5) was evaluated. Magnetic resonance imaging (MRI) revealed a mass originating from the nasopharynx and passing through the petrous apex, foramen lacerum, carvernous sinus, sphenoid sinus, orbital apex, and inferior orbital fissure. The mass had high signals on T2-weighted imaging. After 5 days, the mass was removed by endoscopic surgery and aspergillus was detected histopathologically. The patient was given intravenous voriconazole for 11 days and oral voriconazole for 11 weeks. Ptosis and ocular movement limitation began to improve after 6 weeks postoperatively. After 4 months, ocular movement was not limited and there was no recurrence during the 1 year follow-up period.
CONCLUSIONS
The present case showed that orbital aspergillosis can invade the intracranial area and third, fourth, and sixth nerve palsy can develop without exophthalmos. Thus, when ocular movement disorders, ptosis and symptoms of sinusitis are present in orbital aspergillosis patients, use of appropriate diagnostic tools such as MRI and active treatment are important.
MeSH Terms
Figure
-

Figure 1. At the initial visit, the patient had ptosis of the right eye. However, there was no exophthalmos.

Figure 2. Nine cardinal gaze photographs show total ophthalmoplegia of the right eye.
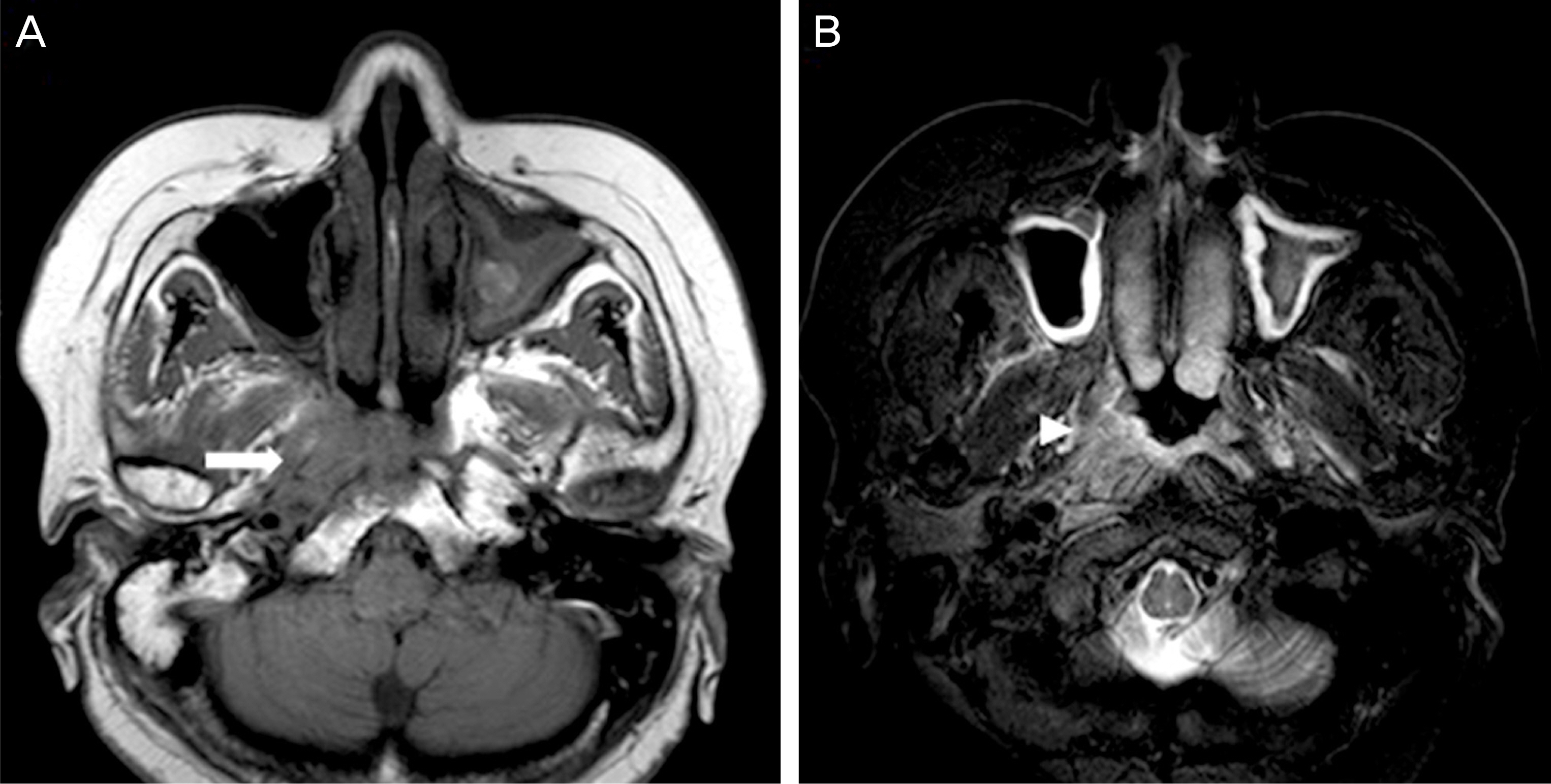
Figure 3. (A) T1-weighted MR image revealed a mass in the right pterygopalatine fossa by low-signal intensity (arrow). (B) The lesion showed high-signal intensity in T2-weighted image (arrowhead).
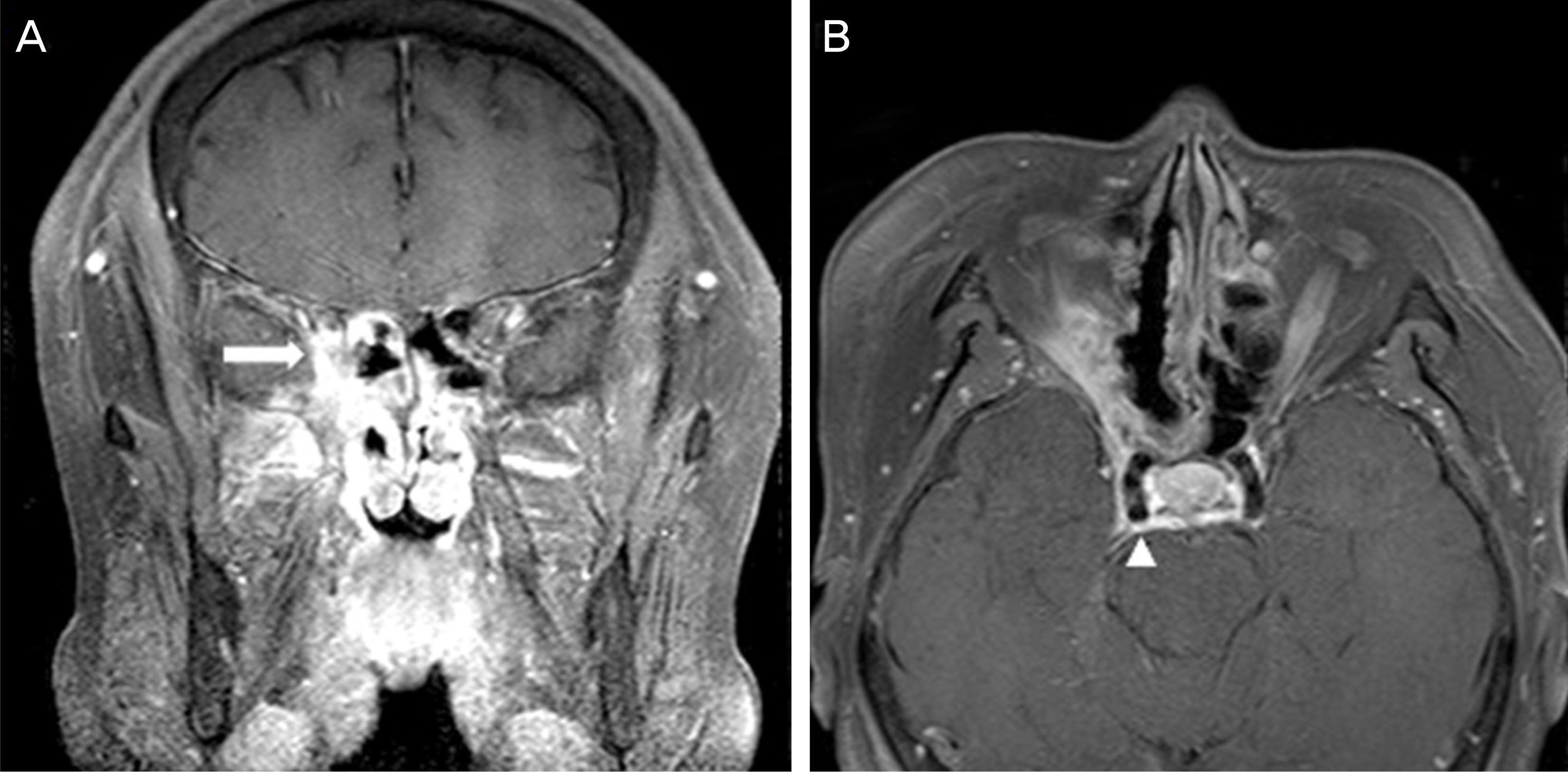
Figure 4. (A) Gadolinium-en-hanced T1-weighted MR image revealed that the mass ex-tended to the right orbital apex and inferior portion of the optic canal with strong enhancement (arrow). (B) The axial view showed an invasion of the right cavernous sinus with peripheral enhancement (arrow- head).
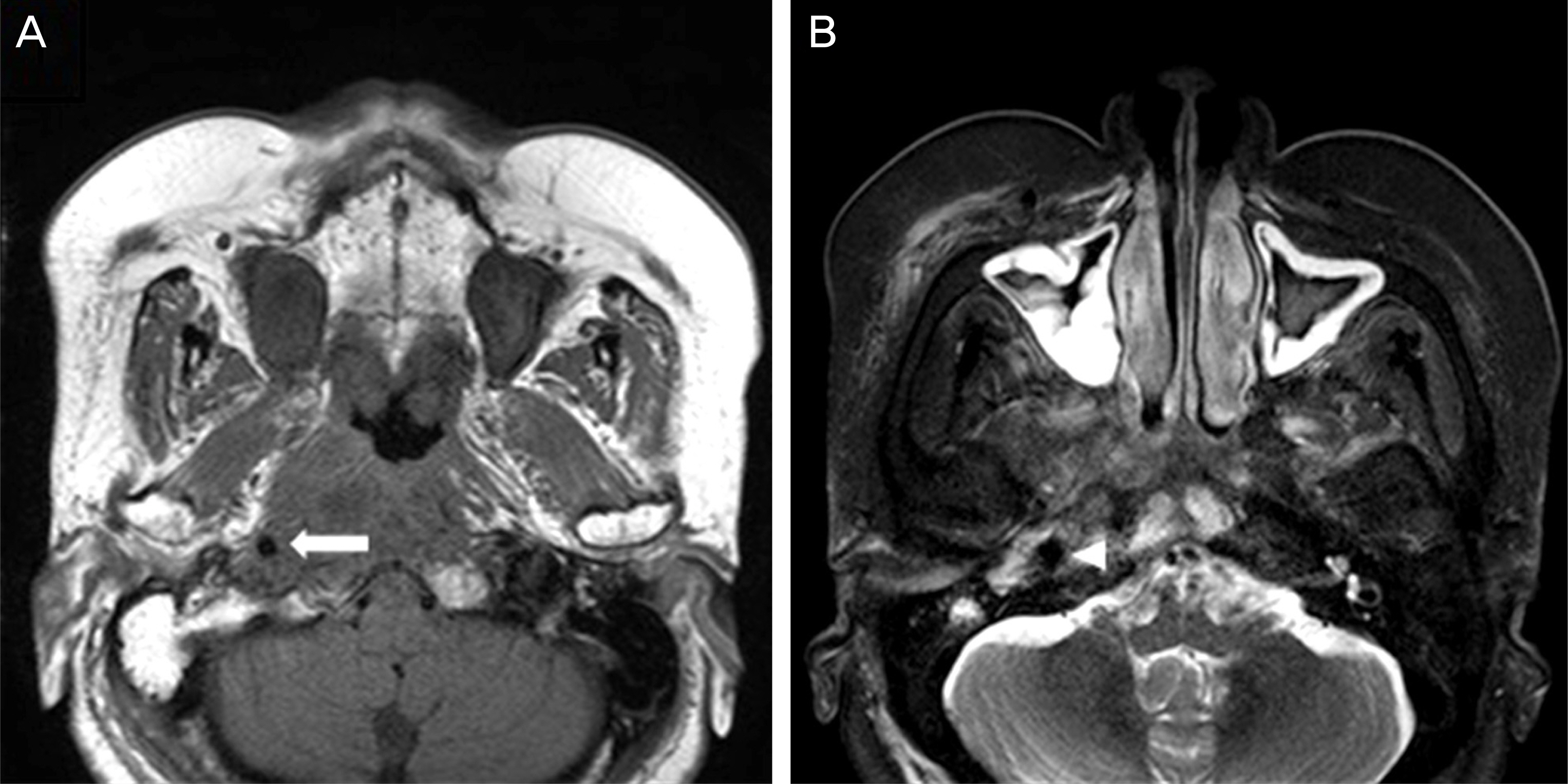
Figure 5. Encasement of the petrous portion of the right internal carotid artery was shown in (A) T1-weighted sequence (arrow) and (B) T2-weighted sequence (arrow- head).
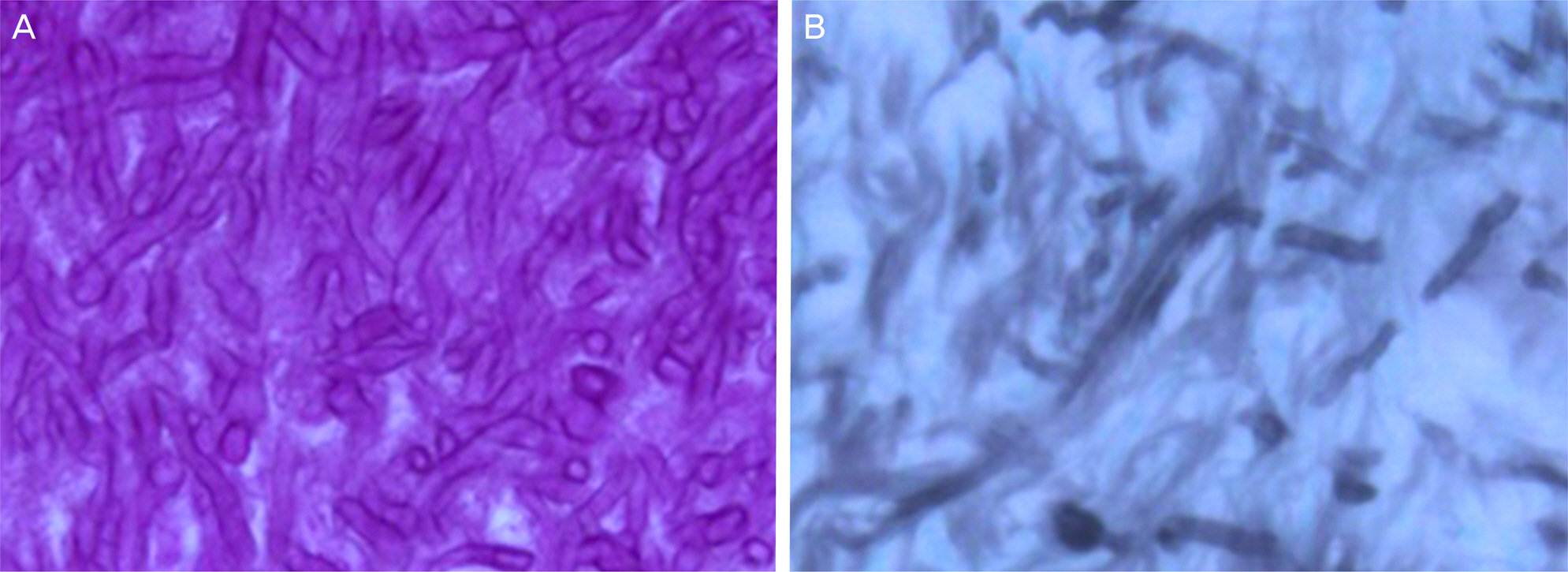
Figure 6. Histologic finding: (A) (PAS stain ×400): Septated fungal hyphae and (B) (GMS stain ×400): Invaded fungal hyphae into the necrotic tissue were found at middle turbinate tissue biopsy.

Figure 7. There was a complete resolution of ocular movement limitation at 4 months after surgery.
Reference
-
References
1. Lim SH, Sung SH, Lim KH. A case of invasive aspergillosis involving the orbital apex and occipital lobe:successful treatment with voriconazole. J Korean Ophthalmol Soc. 2013; 54:540–4.
Article2. Alrajhi AA, Enani M, Mahasin Z, Al-Omran K. Chronic invasive aspergillosis of the paranasal sinuses in immunocompetent hosts from Saudi Arabia. Am J Trop Med Hyg. 2001; 65:83–6.
Article3. Petrick M, Honegger J, Daschner F, et al. Fungal granuloma of the sphenoid sinus and clivus in a patient presenting with cranial nerve III paresis: case report rand review of the literature. Neurosurgery. 2003; 52:955–8. discussion 958-9.4. Lee JC, Lim DJ, Ha SK, et al. Fatal case of cerebral aspergillosis: a case report and literature review. J Korean Neurosurg Soc. 2012; 52:420–2.5. Kim SI, Choi HY, Lee JW. A case of the third nerve palsy in a patient with orbital aspergillosis. J Korean Ophthalmol Soc. 2014; 55:149–54.
Article6. Kim US, Kim JS, Kwon OK, Hwang JM. Complete visual recovery after mycotic aneurysm embolization complicated by cavernous sinus thrombophlebitis. Korean J Ophthalmol. 2010; 24:322–4.
Article7. Yamanoi T, Shibano K, Soeda T, et al. Intracranial invasive aspergillosis originating in the sphenoid sinus: a successful treatment with high-dose itraconazole in three cases. Tohoku J Exp Med. 2004; 203:133–9.
Article8. Mody KH, Ali MJ, Vemuganti GK, et al. Orbital aspergillosis in immunocompetent patients. Br J Ophthalmol. 2014; 98:1379–84.
Article9. Leyngold I, Olivi A, Ishii M, et al. Acute chiasmal abscess resulting from perineural extension of invasive sino-orbital aspergillosis in an immunocompetent patient. World Neurosurg. 2014; 81:203.e1–6.
Article10. Urculo E, Aranzadi MJ, Ruiz I, Villanua J. Aspergillus granuloma of the cavernous sinus: magnetic resonance imaging with patho-logic correlation. Acta Neurochir (Wien). 2005; 147:341–2. discussion 342.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Etiology and Clinical Feature of the Third, Fourth, and Sixth Cranial Nerve Palsy
- Risk Factors and Prognosis of Isolated Ischemic 3rd, 4th, 6th Cranial Nerve Palsy
- A Clinical Study of Paralytic Strabismus
- Neuro-ophthalmologic Evaluation of the Third, Fourth and Sixth Cranial Nerve Paralysis
- Etiology of Isolated Third, Fourth, and Sixth Cranial Nerve Palsies with a Cancer History
