J Korean Ophthalmol Soc.
2014 Dec;55(12):1793-1799. 10.3341/jkos.2014.55.12.1793.
The Clinical Efficacy of the Haigis Formula Using A-Scan Contact Ultrasound Biometry
- Affiliations
-
- 1Department of Ophthalmology, Pusan National University Hospital, Pusan National University School of Medicine, Busan, Korea. jongsool@pusan.ac.kr
- 2Department of Emergency Medicine, The Armed Forces Medical Command, Seongnam, Korea.
- KMID: 2338962
- DOI: http://doi.org/10.3341/jkos.2014.55.12.1793
Abstract
- PURPOSE
To investigate the accuracy of the Haigis formula compared to other formulas using contact ultrasound biometry.
METHODS
This study was performed on 94 patients (114 eyes) who underwent cataract surgery in our hospital. Axial length (AXL) and anterior chamber depth (ACD) were measured using both A-scan and intraocular lens (IOL) Master(R). Patients were divided into three groups based on AXL; Group I (AXL < 22.5 mm), Group II (22.5 mm < or = AXL < 25.5 mm), and Group III (AXL > or = 25.5 mm). Before cataract surgery, predicted refraction was calculated using the Haigis, SRK/T, Hoffer Q, and Holladay 1 formulas using both A-scan and IOL Master(R) measurements. Mean absolute error (MAE) were analyzed at one month after surgery using the various IOL formulas.
RESULTS
Using contact ultrasound biometry, in Group I, MAE of Haigis was 0.80 +/- 0.67 D and was significantly lower than that using SRK/T. In Group II, the Haigis MAE was 0.72 +/- 0.55 D and was significantly lower than the results of all other formulas. In Group III, the Haigis MAE was 0.76 +/- 1.13 D and not significantly different from the results of other formulas. Comparing MAE of A-scan to IOL Master(R), the Haigis formula showed 0.16 D higher error that decreased when the AXL was close to the normal range.
CONCLUSIONS
Using contact ultrasound biometry, the Haigis formula provided the best predictability of postoperative refractive outcome compared to other formulas in eyes with normal axial length.
Keyword
MeSH Terms
Figure
-

Figure 1. The perform ance of various intraocular lens (IOL) calculation formulas with ultrasound biometry. MAE = mean absolute error.
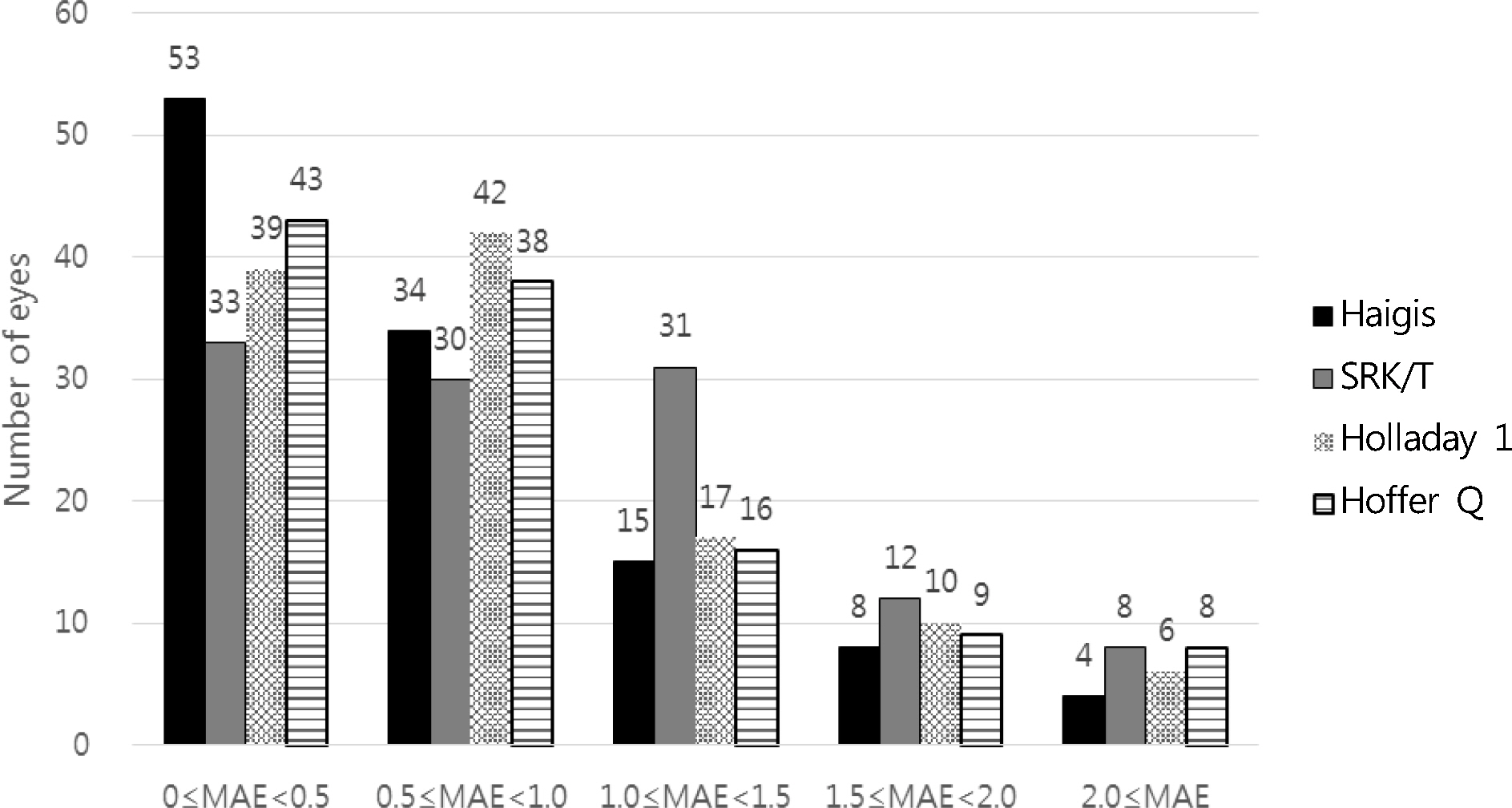
Figure 2. Intraocular lens (IOL) power calculation error using A-scan in the various IOL calculation formulas. MAE = mean absolute error using A-scan (diopter).
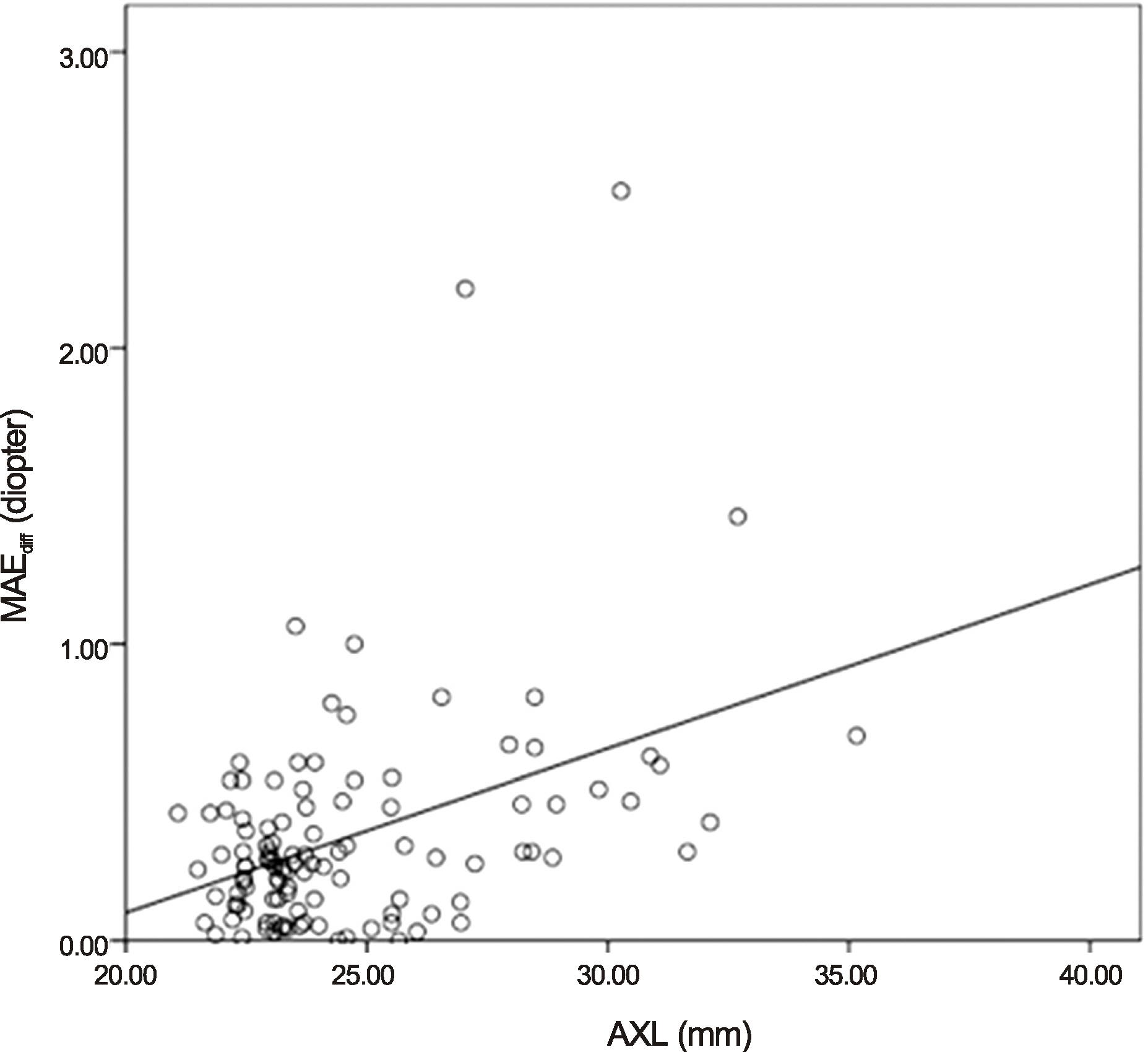
Figure 3. The linear regression analysis of absolute mean absolute error difference between ultrasound and intraocular lens (IOL) Master® using Haigis formula (Linear regression model: R2 = 0.170, p < 0.001). MAEdiff = | MAEA-scan – MAEIOLM |; MAEA-scan = mean absolute error of Haigis formula using A-scan; MAEIOLM = mean absolute error of Haigis formula using IOL Master®; AXL = axial length.
Reference
-
References
1. Olsen T. Prediction of intraocular lens position after cataract extraction. J Cataract Refract Surg. 1986; 12:376–9.
Article2. Olsen T. Sources of error in intraocular lens power calculation. J Cataract Refract Surg. 1992; 18:125–9.
Article3. Bhatt AB, Schefler AC, Feuer WJ, et al. Comparison of predictions made by the intraocular lens master and ultrasound biometry. Arch Ophthalmol. 2008; 126:929–33.
Article4. Choi J, Choi SK. Accuracy of intraocular lens power calculation in diabetic patients. J Korean Ophthalmol Soc. 2010; 51:188–94.
Article5. Tehrani M, Krummenauer F, Blom E, Dick HB. Evaluation of the practicality of optical biometry and applanation ultrasound in 253 eyes. J Cataract Refract Surg. 2003; 29:741–6.
Article6. Giers U, Epple C. Comparison of A-scan device accuracy. J Cataract Refract Surg. 1990; 16:235–42.
Article7. Yi CH, Choi SH, Chung ES, Chung TY. Accuracy of the haigis formula based on axial length and anterior chamber depth. J Korean Ophthalmol Soc. 2011; 52:175–81.
Article8. Haigis W, Lege B, Miller N, Schneider B. Comparison of immersion ultrasound biometry and partial coherence interferometry for intraocular lens calculation according to Haigis. Graefes Arch Clin Exp Ophthalmol. 2000; 238:765–73.
Article9. Eleftheriadis H. IOLMaster biometry: refractive results of 100 consecutive cases. Br J Ophthalmol. 2003; 87:960–3.
Article10. Rose LT, Moshegov CN. Comparison of the Zeiss IOLMaster and applanation A-scan ultrasound: biometry for intraocular lens calculation. Clin Experiment Ophthalmol. 2003; 31:121–4.
Article11. Shin JA, Chung SK. Comparison of the refractive results measured by ultrasound and partial coherence interferometers. J Korean Ophthalmol Soc. 2013; 54:723–7.
Article12. Hwang JS, Lee JH. Comparison of the IOL Master® and A-scan ultrasound: refractive results of 96 consecutive cases. J Korean Ophthalmol Soc. 2007; 48:27–32.13. Hoffer KJ. The Hoffer Q formula: a comparison of theoretic and regression formulas. J Cataract Refract Surg. 1993; 19:700–12.
Article14. Haigis W. The Haigis formula. Shammas HJ, editor. Intraocular lens power calculations. Thorofare, NJ: Slack Inc.;2004. p. 5–57.15. Kim BH, Wee WR, Kim MK. Analysis of factors that influence on accuracy of intraocular lens power calculation. J Korean Ophthalmol Soc. 2014; 55:173–81.
Article16. Dinc UA, Gorgun E, Oncel B, et al. Assessment of anterior chamber depth using Visante optical coherence tomography, slitlamp optical coherence tomography, IOL Master, Pentacam and Orbscan IIz. Ophthalmologica. 2010; 224:341–6.
Article17. Holladay JT, Prager TC, Chandler TY, et al. A three-part system for refining intraocular lens power calculations. J Cataract Refract Surg. 1988; 14:17–24.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Accuracy of Intraocular Lens Power Calculation Formulas in Primary Angle Closure Glaucoma
- Accuracy of the Haigis Formula Based on Axial Length and Anterior Chamber Depth
- Accuracy of Intraocular Lens Power Prediction Using 9 Formula
- Comparison of Intraocular Lens Calculation Formulas Measured by Immersion-Type A-Scan Ultrasound and Partial Coherence Interferometry
- Comparison of Four Systems of IOL Calculation after Keratorefractive Surgery in Eyes Requiring Cataract Surgery
