Cyclocryotherapy and Intravitreal Gas Tamponade of a Chronic Cyclodialysis Cleft: Case Report
- Affiliations
-
- 1Department of Ophthalmology, Gyeongsang National University School of Medicine, Jinju, Korea. stramast@naver.com
- 2Institute of Health Science, Gyeongsang National University, Jinju, Korea.
Abstract
- PURPOSE
To report a case of chronic hypotony maculopathy caused by traumatic cyclodialysis cleft and treated with 20% sulfur hexafluoride (SF6) gas tamponade with cyclocryotherapy.
CASE SUMMARY
A 39-year-old woman with a history of blunt trauma developed a unilateral chronic ocular hypotony in her left eye. She was treated with topical atropine sulphate 1% for 2 months. Three years later, she was referred to our clinic for evaluation and treatment of persistent hypotony. The intraocular pressure (IOP) was 4 mm Hg and the best corrected visual acuity was 0.4. B-scan echography revealed a choroidal effusion and fundus examination showed choroidal detachment and macular folds. Gonioscopy examination revealed cyclodialysis cleft from the direction of 7 o'clock to 11 o'clock. A single bubble of SF6 20% (0.4 cc) was injected into the vitreous cavity and transconjunctival cyclocryotherapy was performed under retrobulbar anesthesia. Six months later, the IOP was 12 mm Hg and the best corrected visual acuity was 1.0. B-scan echograpy and fundus examination showed the disappearance of the choroidal effusion.
CONCLUSIONS
Gas tamponade with cyclocryotherapy may be useful in cases of cyclodialysis cleft that failed to respond to medical therapy.
MeSH Terms
Figure
-

Figure 1 Preoperative examination. (A) Gonioscopy examination revealed cyclodialysis cleft from 7 o'clock to 11 o'clock. (B) Pentacam showed anterior displacement of lens-iris diaphragm and shallow anterior chamber. (C, D) Fundus photograph and B-scan echography revealed a choroidal detachment and macular folds and choroidal effusion. (E) The preoperative optical coherence tomography showed macular edema with chorioretinal folds.
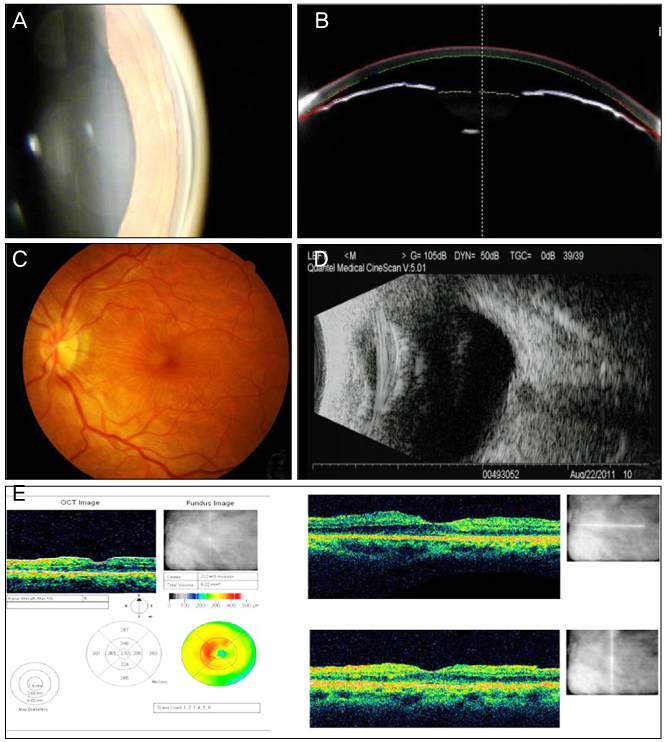
Figure 2 The examinations 6 months after operation. (A) Gonioscopy examination displayed the closure of the cyclodialysis cleft. (B) Pentacam showed the deepening of anterior chamber. (C) Fundus photograph showed disappearance of chorioretinal folds. (D) B-scan echography revealed a loss of choroidal detachment. (E) The postoperative optical coherence tomography showed marked resolution of the chorioretinal folds and serous fluid.
Reference
-
1. Ormerod LD, Baerveldt G, Sunalp MA, Riekhof FT. Management of the hypotonous cyclodialysis cleft. Ophthalmology. 1991. 98:1384–1393.2. Grosskreutz C, Aquino N, Dreyer EB. Cyclodialysis. Int Ophthalmol Clin. 1995. 35:105–109.3. Krohn J. Cryotherapy in the treatment of cyclodialysis cleft induced hypotony. Acta Ophthalmol Scand. 1997. 75:96–98.4. Maumenee AE, Stark WJ. Management of persistent hypotony after planned or inadvertent cyclodialysis. Am J Ophthalmol. 1971. 71(1 Pt 2):320–327.5. Slusher MM. Pseudophakic choroidal detachment with cyclodialysis cyst. Ophthalmic Surg. 1987. 18:191–194.6. Harbin TS Jr. Treatment of cyclodialysis clefts with argon laser photocoagulation. Ophthalmology. 1982. 89:1082–1083.7. Kim CS, Ahn SI, Ahn BH. Treatment for persistent hypotony due to cyclodialysis. J Korean Ophthalmol Soc. 1998. 39:1505–1515.8. Brooks AM, Troski M, Gillies WE. Noninvasive closure of a persistent cyclodialysis cleft. Ophthalmology. 1996. 103:1943–1945.9. Kim KH, Kim JW, Oh TH, Lee DH. Surgical repair of traumatic cyclodialysis with persistent hypotony. J Korean Ophthalmol Soc. 1997. 38:1294–1299.10. Ahn K, Kee C. Clinical manifestations of cyclodialysis cleft and prognostic factors associated with direct cyclopexy. J Korean Ophthalmol Soc. 2003. 44:2328–2335.11. Helbig H, Foerster MH. Management of hypotonous cyclodialysis with pars plana vitrectomy, gas tamponade, and cryotherapy. Ophthalmic Surg Lasers. 1996. 27:188–191.12. Hoerauf H, Roider J, Laqua H. Treatment of traumatic cyclodialysis with vitrectomy, cryotherapy, and gas endotamponade. J Cataract Refract Surg. 1999. 25:1299–1301.13. Ishida Y, Minamoto A, Takamatsu M, et al. Pars plana vitrectomy for traumatic cyclodialysis with persistent hypotony. Eye (Lond). 2004. 18:952–954.14. Kim KH, Song BJ, Choi YI. Hypotony with cyclodialysis after blunt trauma to the eye. J Korean Ophthalmol Soc. 1997. 38:121–128.15. Partamian LG. Treatment of a cyclodialysis cleft with argon laser photocoagulation in a patient with a shallow anterior chamber. Am J Ophthalmol. 1985. 99:5–7.16. Ji YH, Kee CW. A case of traumatic cyclodialysis cleft diagnosed by ultrasound biomicroscopy. J Korean Ophthalmol Soc. 1998. 39:817–822.17. Tate GW Jr, Lynn JR. A new technique for the surgical repair of cyclodialysis induced hypotony. Ann Ophthalmol. 1978. 10:1261–1268.18. McCannel MA. A retrievable suture idea for anterior uveal problems. Ophthalmic Surg. 1976. 7:98–103.19. Kalenak JW, Pulido JS. Pneumatic cyclopexy. Arch Ophthalmol. 1995. 113:558.20. Küchle M, Naumann GO. Direct cyclopexy for traumatic cyclodialysis with persisting hypotony. Report in 29 consecutive patients. Ophthalmology. 1995. 102:322–333.21. Mandava N, Kahook MY, Mackenzie DL, Olson JL. Anterior scleral buckling procedure for cyclodialysis cleft with chronic hypotony. Ophthalmic Surg Lasers Imaging. 2006. 37:151–153.22. Ceruti P, Tosi R, Marchini G. Gas tamponade and cyclocryotherapy of a chronic cyclodialysis cleft. Br J Ophthalmol. 2009. 93:414–416.23. Kim C, Yu HG. Treatment of Hypotony maculopathy caused by traumatic cyclodialysis with vitrectomy, gas tamponade, and cryotherapy. J Korean Ophthalmol Soc. 2006. 47:1691–1695.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Treatment of Hypotony Retinopathy with Cyclodialysis Cleft by Intravitreal Gas Injection
- Novel Adjuvant Method to Assist Localisation of a Cyclodialysis Cleft
- Treatment of Hypotony Maculopathy Caused by Traumatic Cyclodialysis with Vitrectomy, Gas Tamponade, and Cryotherapy
- A Case of Cyclodialysis Cleft Treated with Argon Laser Photocoagulation
- A Case of Cyclodialysis Cleft with Hypotony during Ahmed Valve Implantation Surgery
